Visual Poster SCS – Swiss College of Surgeons Annual Meeting 2026
The Visual Abstracts are displayed on the «Luzerner Terrasse» on the 2nd floor.
All authors are kindly asked to put the Visual Abstracts on display on Thursday morning, 11 June 09:00 until Friday, 12 June 2026 at 14:00 and be present during the poster walk on Friday, 12. June 2026, 09:30 – 10:30, to answer questions from interested colleagues.
Visual Abstracts
Visual Abstracts
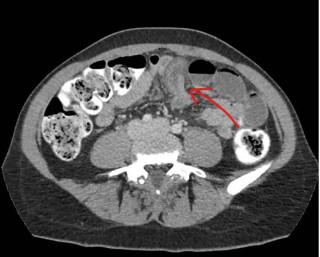
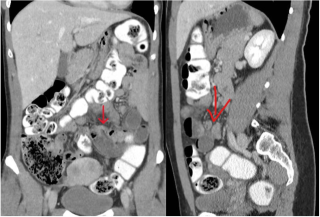
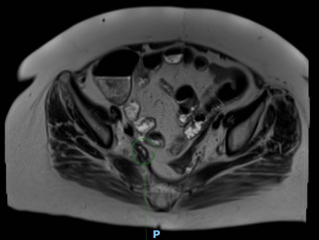
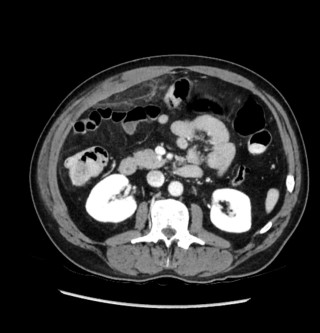
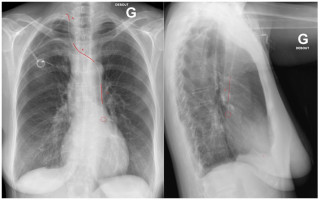
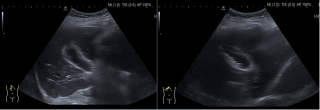
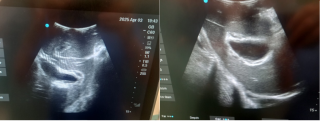
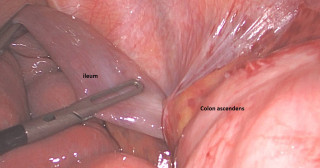
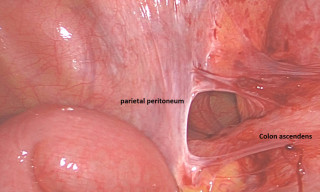
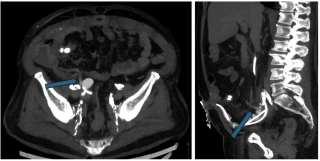
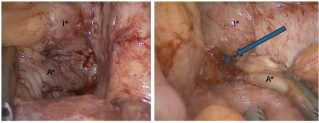
Closed-loop Small Bowel Obstruction through an Internal Hernia caused by Meckel’s Diverticulum: a Case Report
Abstract
Background
Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract, affecting approximately 2–3% of the population, however asymptomatic for most. In adults, internal hernia causing small bowel obstruction is a rare but potentially severe complication.
Several previous case reports have described cases of closed-loop obstruction caused by mesodiverticular bands creating an internal hernia. In a literature review, Unadike et al. reported 16 cases of mesodiverticular band–related obstruction, with high rates of bowel ischemia and resection. Laparotomy was performed in 75% of patients and was associated with ischemic bowel in 58.3% and bowel resection in 83.3% of cases, whereas laparoscopy accounted for 25% of cases, with bowel resection required in half of them.
We report a case of closed-loop small bowel obstruction secondary to Meckel’s diverticulum.
Conclusion
This case highlights an uncommon mechanism of closed-loop small bowel obstruction caused by a Meckel’s diverticulum. Although Meckel’s diverticulum is common, internal herniation with closed-loop obstruction remains rare and difficult to diagnose preoperatively. In young patients with acute small bowel obstruction and no prior abdominal surgery, Meckel’s diverticulum should be considered. Early surgical exploration is essential to prevent ischemic complications.
Case presentation
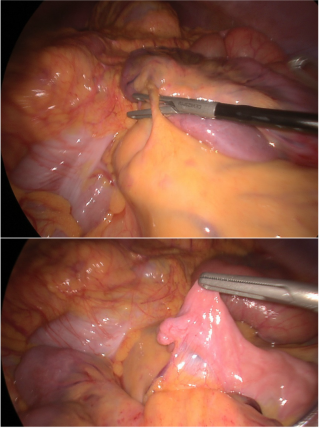
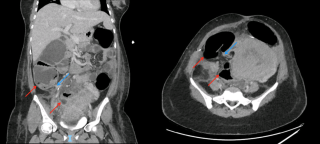
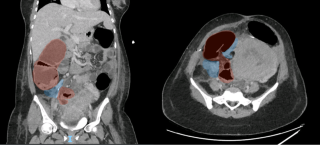
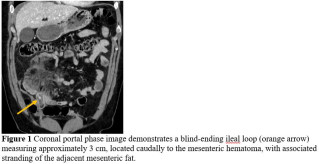
A 31-year-old previously healthy woman, with no surgical history, presented with sudden-onset, severe peri-umbilical abdominal pain unresponsive to high-dose opioids. CT-scan revealed mildly dilated distal jejunum with mesenteric edema and free fluid (Fig. 1, 2). Because of persistent pain despite step III analgesia, emergency diagnostic laparoscopy was performed. Intraoperatively, a closed-loop obstruction of an ileal segment was identified, herniated through a narrow internal window formed by an adherent mesenteric vessel supplying a Meckel’s diverticulum (Fig. 3). The vascular band was divided, releasing the closed loop, with no irreversible small bowel ischemic damage. The Meckel’s diverticulum was resected. The post-operative course was uneventful, and the patient was discharged after two days.
Massive Hemoperitoneum From a Spontaneous Jejunal Intramural Hematoma: A Case Report
Abstract
Background
Spontaneous intramural small bowel hematoma (SISBH) is an acute, non-traumatic accumulation of blood within the intestinal wall, most frequently involving the jejunum. It is mainly associated with anticoagulant therapy and coagulation disorders. Most cases are uncomplicated and can be managed conservatively. Massive hemoperitoneum is exceptionally reported. We report the case of SISBH complicated by massive hemoperitoneum in a patient receiving direct oral anticoagulants (DOACs).
Conclusion
Although SISBH is usually managed conservatively, it may become life-threatening when complicated by massive hemoperitoneum. When associated with hemodynamic instability, SISBH mandates immediate surgical management. In this setting damage control surgery with delayed anastomosis appears as a safe and effective strategy in unstable patients. SISBH should be considered in anticoagulated patients with abdominal pain and anemia.
Case presentation
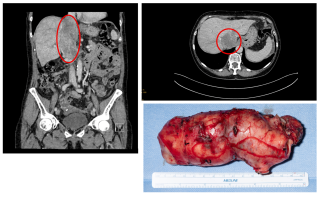
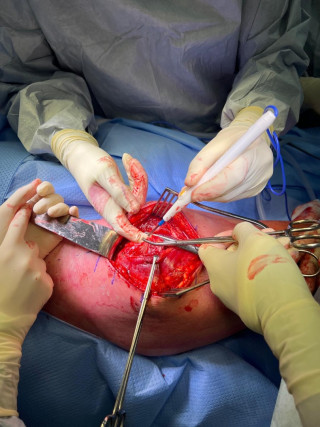
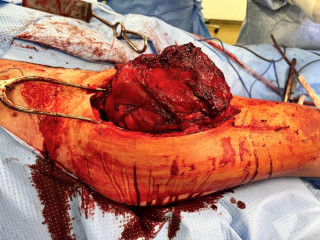
A 37-year-old man with an history of cirrhosis and atrial fibrillation treated with apixaban was admitted for weakness and dizziness. On admission, he was hypotensive and tachycardic, with signs of peripheral hypoperfusion and diffuse abdominal tenderness. Laboratory investigations revealed severe anemia (Hb 46 g/L), marked coagulopathy, and metabolic acidosis with elevated lactate levels. Abdominal CT scan demonstrated a left flank mesenteric lesion exerting mass effect on adjacent small bowel loops, associated with a large-volume acute hemoperitoneum. Emergency exploratory laparotomy revealed approximately 4 liters of hemoperitoneum and a large jejunal intramural hematoma with complete serosal rupture. Segmental jejunal resection was performed with temporary abdominal closure. A planned second-look laparotomy allowed jejunojejunal anastomosis. Histopathological examination confirmed a submucosal hematoma with preserved mucosa and no evidence of ischemia.


Uretero-Colonic Fistula in the Setting of Rectal Adenocarcinoma: A Case Report
Abstract
Background
Uroenteric fistulas are abnormal communications between the urinary tract and the gastrointestinal tracts. Colovesical fistulas are the most common subtype, typically secondary to diverticular disease. In contrast, uretero-colonic fistulas are exceedingly rare, accounting for fewer than 0.5% of colorectal surgical cases, with only sporadic cases reported in the literature. Reported etiologies include colorectal malignancy, prior pelvic surgery, radiotherapy, chronic inflammatory conditions, diverticular disease, and prolonged ureteral stenting. Clinical presentation is often nonspecific, frequently characterized by recurrent urinary tract infections or pyelonephritis. Diagnosis is challenging and typically requires cross-sectional imaging and retrograde ureteropyelography. Management is not standardized and usually necessitates a multidisciplinary approach. We present a rare case of a right-sided uretero-colonic fistula occurring after multimodal treatment for rectal adenocarcinoma and provide a brief review of the literature.
Conclusion
Uretero-colonic fistulas are rare but potentially severe complications, particularly in patients with prior pelvic malignancy, radiotherapy, and prolonged ureteral stenting. Recurrent urinary tract infections caused by enteric pathogens or pneumaturia should raise clinical suspicion for a uroenteric fistula. Combined cross-sectional imaging with retrograde ureterography are essential for diagnosis and surgical management should aim at fistula eradication and preservation of renal function.
Case presentation
A 65-year-old woman with rectal adenocarcinoma (pT4bN0R2, KRAS-mutated) treated with neoadjuvant chemoradiotherapy, and extensive pelvic surgery developed chronic right-sided ureteral obstruction requiring long-term ureteral stenting. From 2023 onward, she experienced recurrent episodes of pyelonephritis, with urine cultures repeatedly isolating enteric organisms. In 2025, pelvic magnetic resonance imaging and retrograde ureteropyelography revealed right-sided hydronephrosis and a fistulous tract connecting the distal right ureter and the rectosigmoid colon, without evidence of tumor recurrence. Surgical management consisted of a bloc resection of the fistula, proctectomy with perineal closure, right ureteral reimplantation, terminal colostomy, and omentoplasty. The postoperative course was uneventful.


Idiopathic Segmental Infarction of the Greater Omentum (ISIGO): A Case Report
Abstract
Background
Idiopathic segmental infarction of the greater omentum (ISIGO) is a rare cause of acute abdominal pain and often mimics common surgical emergencies, while systemic signs may be absent or mild. Contrast-enhanced computed tomography (CT) is the key modality for diagnosis and can allow initial conservative management in selected stable patients. However, treatment failure may occur and require surgery.
Conclusion
ISIGO should be included in the differential diagnosis of acute abdominal pain. Current evidence supports conservative treatment in stable patients with confirmed CT diagnosis, but failure occurs in a minority and warrants laparoscopy, particularly with persistent symptoms or diagnostic uncertainty.
Case presentation
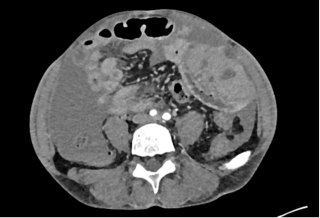
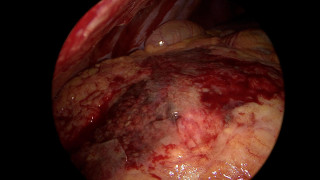
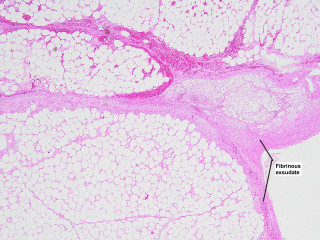
A 55-year-old overweight man presented with one week of right-sided abdominal pain with recent worsening despite outpatient medical therapy. He was hemodynamically stable but had right upper quadrant tenderness and localized guarding. Laboratory testing showed elevated C-reactive protein with a normal leukocyte count and normal liver biochemistry. CT demonstrated inflammatory fat stranding of the right greater omentum with a hyperdense rim, consistent with right-sided omental infarction (Figure 1). Because pain persisted despite conservative management, diagnostic laparoscopy was performed and confirmed ischemic omentum with hemorrhagic peritoneal fluid (Figure 2), and a normal gallbladder and appendix. Laparoscopic omentectomy was completed without complications. Histopathology confirmed omental infarction (Figure 3). The patient was discharged on postoperative day 1 and remained asymptomatic at 6-week follow-up.
Complete Bilateral Spontaneous Pneumothorax at Moderate Altitude Revealing Marfan Syndrome: A Case Report
Abstract
Background
Primary spontaneous pneumothorax is frequently encountered in young adults. However, simultaneous complete bilateral pneumothorax is rare and potentially fatal. Exposure to altitude-related barometric pressure changes may precipitate pneumothorax in susceptible individuals, particularly those with unrecognized connective tissue disorders.
Conclusion
This case illustrates complete bilateral spontaneous pneumothorax as a dramatic sentinel event revealing Marfan syndrome, likely precipitated by moderate altitude exposure. It emphasizes the importance of comprehensive etiological evaluation in young patients with severe or atypical pneumothorax and highlights the value of early multidisciplinary management to prevent life-threatening complications.
Case presentation
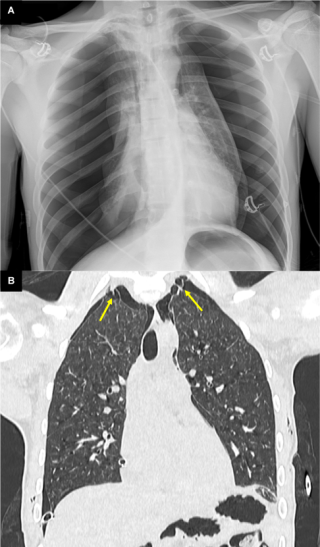
We report the case of a 17-year-old previously healthy male who developed sudden severe dyspnea while recreational skiing at a moderate altitude of 2'200 meters. On-site emergency management required immediate bilateral needle decompression, followed by urgent transfer to hospital care. Imaging confirmed a complete bilateral pneumothorax with bilateral apical subpleural blebs (Figure 1). Sequential bilateral chest tube placement was performed, and the patient subsequently underwent staged bilateral video-assisted thoracoscopic surgery with apical wedge resection and mechanical pleurodesis. Postoperative recovery was uneventful, with no recurrence during follow-up. Etiological investigations revealed normal alpha-1 antitrypsin levels. Transthoracic echocardiography identified a bicuspid aortic valve associated with moderate aortic regurgitation (grade 2/4). Combined clinical, radiological, and cardiac findings ultimately led to the diagnosis of Marfan syndrome, previously unrecognized.
Spoliative ileal tumor revealing Peutz-Jegher Syndrome
Abstract
Background
Peutz-Jegher Syndrome (PJS) is an autosomal dominant inherited disease. It is characterized by the development of mucocutaneous pigmentations and gastrointestinal hamartomatous polyps. Predominantly found in the small intestine, those polyps can typically lead to intussuception and/or bleeding. PJS increase the risk of colorectal, pancreatic, gastric and breast cancers. From a proportional perspective, 1:50’000 to 1:200’00 person is affected by PJS. Due to the rarity of the syndrome, a lack of guidelines exists. For this reason, the follow up is guided by expert consensus.
Conclusion
PJS is a rare but potentially serious disease. If hamartomous polyp associated with pigmentated spots are found, PJS will be the most likely diagnosis. Endoscopic resection is the preferred method, but sometimes, as in our case, surgery is necessary either for large polyps or if they cannot be reached by endoscopy. A consistent follow up and family council could improve long terms outcomes and reduce cancer-induced morbidity and mortality.
Case presentation
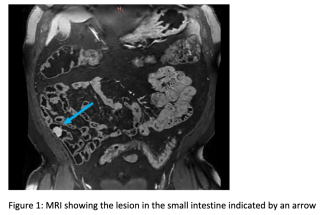
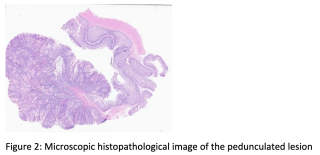
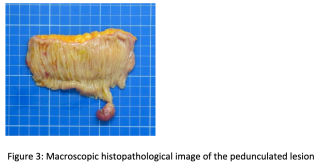
A 60 year old man presented with spoliative anemia. He is not known for cutanous macules around the mouth. An initial work up by colonoscopy and gastroscopy revealed a Helicobacter pylori infection without other significant abnormalities. Subsequently, a magnetic resonance imagery was performed and a 18 mm polyp located in the small intestine was identified (Figure 1). The lesion was not reachable by conventional endoscopy techniques. As endoscopic resection was not feasible, the patient underwent an explorative laparoscopy which enabled the discovery of a lesion in the terminal ileum coupled with an intussuception. The histopathological examinations demonstrated a pedunculated polypoid lesion, measuring 2 x 1.7 cm with a pedicle measuring 2.4 cm consistent with a Peutz-Jegher Syndrome (Figure 2 and Figure 3). Multidisciplinary meeting proposed genetic counselling and endoscopic follow up.
Rare Benign Tumors of the Distal Phalanx: A Case Series of Eight Distinct Entities
Abstract
Background
The distal phalanx may be affected by a broad spectrum of benign soft-tissue and bone tumors, posing a diagnostic challenge due to their rarity and diverse histopathological origins. Accurate diagnosis is essential for appropriate surgical management.
Aims
We present an image-based overview of eight benign soft-tissue and bone tumors affecting the distal phalanx through a surgical case series.
Methods
A retrospective case series of eight patients with benign soft-tissue and bone tumors of the distal phalanx were reviewed. The patients were treated by a single surgeon between 2011 and 2025. The entities included acral fibromyxoma, fibrokeratoma, subungual glomus tumor, glomus tumor of the pulp, ossifying fibromyxoid tumor of the distal interphalangeal joint, subungual mucoid cyst, volar exostosis of the distal phalanx, and enchondroma.
Clinical presentation, imaging findings, histopathological characteristics, surgical techniques, and follow-up outcomes were evaluated (Figures 1–3).
Results
Preoperative clinical assessment combined with lesion-oriented imaging enabled comprehensive characterization of all lesions and supported surgical planning. Four patients exhibited nail deformities. Surgical excision was performed in all cases with histopathological confirmation. No major complications were observed during follow-up.
Correlation of clinical appearance, imaging findings, and histopathology enabled the creation of a structured, image-based overview illustrating eight benign soft-tissue and bone tumors of the distal phalanx.
Conclusion
Rare tumors of the distal phalanges require careful clinical evaluation and imaging assessment to ensure accurate diagnosis. Surgical excision with histopathological confirmation remains the treatment of choice in these tumors.



Sigmoid Colon Obstruction from Broad Ligament Internal Herniation After Cesarean Section: A Case of Successful Endoscopic Reduction
Abstract
Background
Internal herniation through a defect of the broad ligament is an uncommon cause of bowel obstruction, typically involving the small intestine. Colonic involvement is exceptionally rare. Early diagnosis in the postpartum period is often difficult, as symptoms can mimic expected postoperative findings. This case describes an unusual sigmoid colon herniation occurring shortly after cesarean section and successfully treated by endoscopic reduction.
Conclusion
Sigmoid colon herniation through the broad ligament is an exceptional postpartum complication. In the absence of ischemia and when the herniated segment is accessible endoscopically, endoscopic reduction may represent a safe and effective conservative strategy, avoiding reoperation in the early postoperative setting. This case expands the spectrum of broad ligament hernias and suggests that carefully selected patients may benefit from nonoperative management.
Case presentation
A 34 year-old postpartum patient developed acute abdominal pain, distension, and inflammatory syndrome on postoperative day 3 following cesarean section. Abdominopelvic CT revealed an incarcerated sigmoid loop herniating through the right broad ligament without signs of ischemia. An interdisciplinary discussion led to attempted endoscopic management with laparoscopic standby. Colonoscopy demonstrated a luminal stenosis corresponding to the herniation site, without ischemic changes. Gentle advancement of the endoscope combined with external manual pressure allowed complete reduction of the herniated segment. Full sigmoidoscopic reevaluation confirmed absence of ischemia. Surgical intervention was therefore avoided. Bowel function returned the following day, inflammatory markers normalized, and the postoperative course was uneventful. No recurrence or symptoms related to the ligament defect were observed during 8-month follow-up.
Ileocecal resections for Crohn's: Predictive value of resection margins on the risk of re-surgery in the Swiss IBD Cohort
Abstract
Background
The ileocecal region is the most common primary site of Crohn’s disease, and up to 90% of patients will require an ileocecal resection during their lifetime. The impact of positive resection margins on postoperative surgical recurrence remains controversial in patients undergoing ileocecal resection for Crohn’s disease.
Aims
This study aimed to assess the impact of resection margin status on endoscopic and surgical recurrence following ileocecal resection for Crohn’s disease in a national Swiss cohort.
Methods
A retrospective analysis of the prospective Swiss Inflammatory Bowel Disease Cohort Study (SIBDCS) database was conducted. All consecutive patients who underwent ileocecal resection between 2006 and 2020 with available surgical and pathology reports were included. Endoscopic recurrence was defined as lesion seen at the colonoscopy control according to Rutgeer’s score. Surgical recurrence was defined as the need for bowel surgery after primary ileocecal resection. The primary outcome was surgical recurrence. The secondary outcome was the evaluation of pathology report content with the aim of proposing a standardized pathology report for Crohn’s disease surgery.
Results
A total of 82 patients were included. The median follow-up was 8 years. Positive small bowel resection margins were significantly associated with surgical recurrence (p=0.022) but not with endoscopic recurrence. Pathology reports lacked standardization, did not report resection margin status in 13% of cases, and frequently omitted key histopathological features such as myenteric and submucosal plexitis.
Conclusion
Positive small bowel margins are associated with and increased risk of surgical recurrence. Pathology reports in Switzerland are still lacking important information and should be standardized in order to stratify the postoperative risk of recurrence.
Septic bursitis olecrani caused by Nocardia farcinica in an immunocompromised patient - case report and scoping literature review
Abstract
Background
Septic bursitis is mainly caused by Staphylococcus aureus and Streptococcus spp. However, patients with immunosuppression may experience infections by rare pathogens. Here, we describe a case of septic olecranon bursitis caused by Nocardia farcinica and provide a literature review of musculoskeletal infections by this pathogen.
Conclusion
This report highlights the importance for clinicians to consider rare pathogens in immunosuppressed patients with bursitis, especially when presenting with atypical courses. Localized musculoskeletal infections by Nocardia are mostly treated by a combined surgical and antibiotic approach. Antibiotics are typically administered for one to six months. In case of surgical removal, a shorter antibiotic treatment duration seems sufficient. A multidisciplinary approach involving infectious diseases specialists, microbiologists and surgeons is critical to achieve good outcomes.
Case presentation
A 75-year-old immunosuppressed patient with seronegative rheumatoid arthritis experienced an elbow trauma, followed by a two-week history of progressive painful swelling, slight erythema and finally the formation of a fistula draining cloudy fluid. Culture of the aspirated bursal fluid yielded slow-growing yellow pigmented colonies identified as Nocardia farcinica. Whole genome sequencing confirmed the species without detecting any known virulence genes or resistance mutations. Clinical and radiological evaluation showed no signs of systemic dissemination. The patient was treated by surgical bursectomy and by targeted antimicrobial therapy with oral trimethoprim/sulfamethoxazole. After 3 weeks, the patient developed a systemic allergic reaction, necessitating a switch to susceptibility-guided amoxicillin/clavulanate. Treatment was continued for 3 months, ultimately resulting in the successful complete resolution of the bursitis.
Conservative Management of Degenerative Rotator Cuff Tears: A Systematic Review of Long-Term Clinical Outcomes and Cost Effectiveness
Abstract
Background
Degenerative rotator cuff tears are a common cause of shoulder dysfunction in adults. The optimal choice between conservative management and surgical repair remains controversial, particularly in older patients and in cases of partial-thickness tears.
Aims
This systematic review evaluates long-term clinical outcomes and cost-effectiveness of conservative treatment strategies compared with surgical repair.
Methods
A comprehensive literature search was performed in PubMed, Embase, Cochrane Library, and Scopus for studies published between 2010 and 2025. Randomized controlled trials and cohort studies comparing conservative and surgical interventions for degenerative rotator cuff tears were included. Methodological quality was assessed using the Cochrane Risk of Bias 2 tool and ROBINS-I. Due to heterogeneity in study design and outcome reporting, a meta-analysis was not feasible; therefore, a structured narrative synthesis was conducted. Recent evidence, including emerging conservative modalities such as platelet-rich plasma (PRP) and extracorporeal shockwave therapy (ESWT), was incorporated.
Results
Seven high-quality studies involving 893 patients were included. Conservative treatment, predominantly physiotherapy-based, achieved clinical outcomes comparable to surgery in partial-thickness tears and in low-demand or elderly patients. In contrast, surgical repair demonstrated superior long-term improvements in Constant-Murley Score, Visual Analogue Scale pain scores, American Shoulder and Elbow Surgeons scores, and patient satisfaction in full-thickness tears. Structural re-tears were observed after surgery; however, these did not consistently correlate with inferior functional outcomes, indicating that anatomical integrity does not always predict clinical success. Conservative management was consistently associated with lower direct and indirect healthcare costs across studies. Adjunctive therapies such as ESWT and PRP showed promising benefits in selected patient populations.
Conclusion
Conservative management represents an effective and cost-efficient first-line treatment for degenerative rotator cuff tears, particularly in partial tears and older patients. Surgical repair provides superior long-term functional outcomes in full-thickness tears. Treatment decisions should be individualized based on tear severity, patient activity level, and therapeutic objectives.
Timing Matters: Early Orthoplastic Coverage reduces Fracture-related Infections in Gustilo III B/C Tibial Fractures – A Systematic Review and Meta-Analysis
Abstract
Background
Gustilo-Anderson type III B/C open tibial fractures are among the most complex and high-risk injuries in trauma care. Their management demands a multidisciplinary approach, and early intervention is critical. While early debridement has been established as essential, the optimal timing for definitive orthoplastic coverage remains less clearly defined.
Aims
To evaluate whether early orthoplastic coverage reduces the risk of fracture- related infections (FRIs) and complication rates compared to late coverage in type III B/C open tibial fractures.
Methods
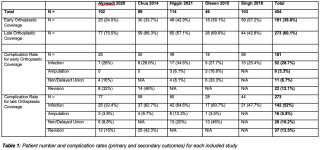
We conducted a PRISMA-compliant systematic review and meta-analysis of studies comparing early versus late orthoplastic treatment in patients with Gustilo-Anderson III B/C open tibial fractures (Table 1). Databases included PubMed and EMBASE. Primary outcome was FRI; secondary outcomes included amputation, non-union, and revision surgery rates. Risk of bias was assessed using the Newcastle-Ottawa Scale.
Results
Of 3007 studies screened, five studies with a total of 454 patients met the inclusion criteria. Cutoff for early vs late treatment was defined variably across studies (either within 72 or 168 hours). Meta-analysis showed that early treatment significantly reduced the odds of infection (OR: 0.34; 95% CI: 0.23–0.52; p < 0.001) compared to late treatment (Table 2).
Subgroup analyses confirmed consistent benefits regardless of timing cutoffs or surgical approach (“fix and flap” vs. staged). While trends suggested reduced rates of amputation and non-union with early treatment, these did not reach statistical significance.
Conclusion
Early orthoplastic coverage significantly reduces FRI in patients with Gustilo- Anderson III B/C open tibial fractures. While secondary outcomes showed positive trends, further high-quality prospective studies are needed.

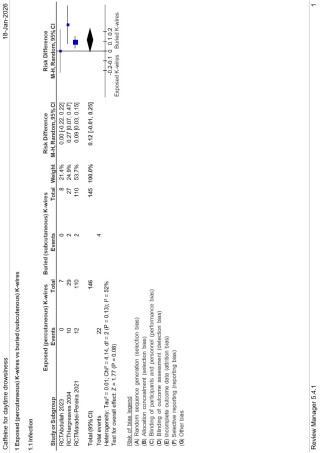
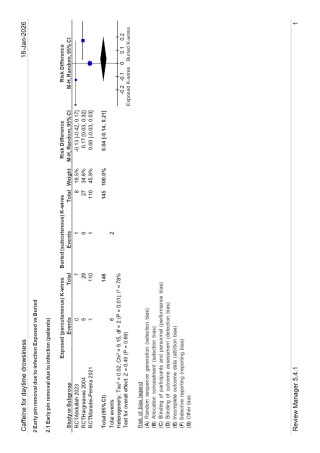
Buried Versus Exposed Kirschner Wires in Distal Radius Fractures: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Background
Percutaneous Kirschner wire fixation remains a common treatment for distal radius fractures. Whether wires should be left exposed or buried subcutaneously is controversial, particularly with regard to infection risk and subsequent clinical consequences.
Aims
To compare exposed versus buried Kirschner wire fixation in distal radius fractures with respect to pin tract infection and clinically relevant secondary outcomes.
Methods
A systematic review and meta-analysis was conducted in accordance with established methodological standards. Randomized controlled trials comparing exposed and buried Kirschner wires for distal radius fracture fixation were included. The primary outcome was pin tract infection, defined as superficial or deep infection. Secondary outcomes were early pin removal due to infection. Risk differences (RD) with 95% confidence intervals (CI) were calculated using random-effects models. Statistical heterogeneity was assessed using the I² statistic.
Results
Three randomized controlled trials comprising 291 patients were included. Buried Kirschner wires were associated with a significantly lower risk of pin tract infection compared with exposed wires (RD 0.12; 95% CI 0.06–0.18; p = 0.0002), with moderate heterogeneity (I² = 52%). There was no statistical difference in early pin removal due to infection in the exposed vs in the buried K-wire group.
Conclusion
Buried Kirschner wires significantly reduce the risk of pin tract infection compared with exposed wires. However, this reduction does not translate into a statistically significant decrease in early wire removal due to infection. From a clinical perspective, the choice between buried and exposed wires may therefore have limited impact on patient-relevant outcomes beyond infection rates and should be individualized based on surgical context and resource considerations.


Use of Sural Artery–Based Flaps in Reconstruction of Distal Lower Extremity Injuries Following Armed Conflict
Abstract
Background
Ongoing armed conflict has resulted in a substantial number of combat-related injuries, with mine-blast trauma to the distal lower extremities being particularly prevalent. These injuries are frequently associated with extensive soft-tissue defects and compromised local vascularity, posing significant reconstructive challenges. Sural artery–based flaps represent a reliable option for soft-tissue coverage due to their consistent vascular anatomy, versatility, and relative technical simplicity.
Aims
To evaluate the effectiveness of sural artery–based flaps in the reconstruction of distal lower extremity defects following mine-blast injuries.
Methods
A narrative review of the PubMed database was conducted alongside a retrospective analysis of clinical and statistical data from patients treated at a local hospital in Ukraine.
Results
Sural artery–based flaps include skin, subcutaneous tissue, fascia, sural nerve, medial superficial sural artery, and the small saphenous vein. Distal sural flaps are characterized by a distally located pedicle with retrograde perfusion via anastomoses between the superficial sural artery and perforators from the fibular artery. Proximal sural flaps utilize an antegrade blood supply with a proximally located pedicle. In cases where local flap elevation on the injured limb was contraindicated due to extensive tissue damage, cross-leg sural flaps were employed.A total of 21 reconstructions were performed: 4 proximal sural flaps, 9 distal sural flaps, and 8 cross-leg flaps. Postoperative complications occurred in 4 cases and were predominantly associated with the severity of blast-related tissue damage and trauma-induced microcirculatory impairment.
Conclusion
Sural artery–based flaps provide an effective and dependable method for reconstruction of distal lower extremity defects in patients with mine-blast injuries. The favorable success rate and low incidence of complications support their use as a valuable reconstructive option in the management of complex combat-related trauma.
Influence of Physiologic Media on Biomechanical Performance of 1.5-mm Wire Cerclages: Defining the Minimum Number of Twists Required for Stability
Abstract
Background
Wire cerclages remain an important adjunct for treating long-bone spiral and peri-implant fractures. However, biomechanical testing is commonly performed under dry laboratory conditions that poorly reflect the physiologic environment. This study evaluated the influence of testing medium on the biomechanical performance of 1.5-mm wire cerclages and determined the minimum twist number required for optimal static and cyclic properties.
Aims
To assess the effect of dry versus physiologic testing environments on cerclage biomechanics and to identify the optimal number of wire twists.
Methods
Using a standardized mechanical setup within a 37 °C heated water bath, cerclage constructs with 4, 6, 8, or 10 twists (n = 6 per group) were created and tested in dry, saline, or fat environments; fat was actively applied during twisting. Static testing evaluated stiffness, load to yield, and load to failure. Separate constructs underwent cyclic tensile testing at 700 N to determine cycles to 2-mm, 3-mm, and 5-mm elongation and cycles to failure
Results
The testing environment significantly influenced all biomechanical parameters. Stiffness increased from 4-8 twists across all media, with no further increase at 10 twists. Load-to-failure peaked at 8–10 twists in each environment. Dry testing consistently yielded higher stiffness, load capacity, and fatigue endurance than saline or fat, markedly overestimating performance. For example, dry constructs with 6 twists achieved 45321±28114 cycles to 2-mm elongation, compared with 18769±15361 cycles in saline and 12306±6838 cycles in fat (p<0.001). Saline and fat showed comparable, consistently inferior performance relative to dry testing, but both improved with increasing twist number. Across all environments, 8 twists provided the most reliable balance of stiffness, strength, and cyclic durability, with no meaningful benefit from additional twists.
Conclusion
Wire cerclage biomechanics are strongly dependent on the surrounding medium. Dry testing substantially overestimates strength and fatigue resistance compared with physiologic saline and fat conditions. At least 8 twists are required for biomechanically robust constructs, and future studies should incorporate physiologic testing environments to better reflect clinical performance.
Sonication of Orthopaedic Implants: Impact of Implant Size, Container Dimensions, and Sonication Time on Bacterial Recovery
Abstract
Background
Sonication enhances detection of implant-associated infections by releasing biofilm-embedded bacteria from orthopaedic hardware. Although a ≥50 CFU/mL diagnostic threshold is often applied in fracture-related infection (FRI), its validity remains uncertain. The influence of implant size, container characteristics, and sonication duration on bacterial recovery is insufficiently defined.
Aims
To determine whether implant size and sonication container volume or material affect the efficiency of bacterial detachment and recovery, using Staphylococcus aureus MU12 and Staphylococcus epidermidis 12.1 as model organisms.
Methods
Titanium locking compression plates (LCP; 577.8 mm²) and titanium TPLO plates (2224.47 mm²) were inoculated with S. aureus or S. epidermidis for 30 min. Implants were sonicated for 1, 2, 5, or 10 min in small (0.47 L), medium (0.60 L), or large (1.0 L) plastic containers, and in small (0.38 L), medium (0.63 L), or large (1.0 L) glass containers. Sonication was performed at 40 kHz and 0.1 W/cm². Bacterial recovery was quantified as CFU/mL. Statistical analysis used two-way ANOVA (P < 0.05).
Results
In small plastic containers, TPLO plates yielded significantly higher bacterial loads than LCP plates (4.07 × 10⁴ ± 1.21 × 10⁴ vs. 1.22 × 10⁴ ± 7 × 10³ CFU/mL; P < 0.01), reflecting surface-area–dependent colonisation. Container size showed no significant effect on recovery (P > 0.05). Glass containers produced slightly higher bacterial counts overall, reaching significance only when compared with small plastic containers (P < 0.05). Increasing sonication duration consistently enhanced bacterial retrieval, with 10 min yielding significantly higher counts than 1 min (5.97 × 10⁴ ± 2.27 × 10⁴ vs. 1.22 × 10⁴ ± 7 × 10³ CFU/mL; P < 0.0001).
Conclusion
Implant surface area and sonication duration substantially influence bacterial recovery, whereas container size and material play minor roles. These findings highlight variability in sonication outcomes and suggest that a fixed CFU threshold for diagnosing FRI may be unreliable. Standardised, evidence-based sonication protocols are required to improve diagnostic consistency and sensitivity.
Clinical equipoise as inclusion criterion: a new way to prevent confounding in observational surgical studies.
Abstract
Background
Observational studies are crucial in orthopedic trauma surgery when randomized controlled trials (RCTs) are not feasible. However, they are susceptible to confounding by indication, as treatment decisions are often influenced by patient characteristics that also affect outcomes. While statistical adjustments are frequently used, they cannot account for unmeasured confounders. Clinical equipoise—defined as genuine uncertainty among experts regarding the optimal treatment—has been proposed as an inclusion criterion to improve baseline comparability in observational studies.
Aims
This study investigates whether higher levels of expert disagreement, as a proxy for clinical equipoise, are associated with improved baseline comparability between treatment groups in patients with proximal humerus fractures.
Methods
We used data from the LADON Humerus study, a multicenter, prospective cohort including patients treated operatively or non-operatively in five hospitals in the Netherlands and Switzerland. An international expert panel of trauma surgeons assessed anonymized cases, blinded to the actual treatment, and recommended a preferred approach. Disagreement between the treatment given and the expert recommendations was categorized into four levels (A: complete disagreement, B: partial, C: minimal, D: complete agreement). Standardized differences (StDiff) for age, sex, ASA score, and AO classification were used to assess comparability between treatment groups across disagreement levels.
Results
A total of 745 patients were evaluated. Comparability between treatment groups improved as the level of disagreement increased. At complete disagreement (Level A), the groups were well balanced in terms of age, sex, and ASA score (StDiff ≤ 0.1). AO classification showed less improvement. Narrower inclusion criteria led to better balance but smaller sample sizes.
Conclusion
Using expert panel disagreement as a clinical equipoise criterion can enhance group comparability in observational research. This approach offers a feasible alternative to randomization and may reduce confounding when RCTs are not possible.
Surgical Patient Safety During the COVID-19 Pandemic: An Integrative Review
Abstract
Background
The COVID-19 pandemic imposed sudden and profound changes on surgical practice worldwide, significantly impacting decision-making and patient safety. The lack of prior knowledge about the disease, combined with limited resources and shortages of personal protective equipment (PPE), challenged healthcare systems and required rapid adaptation of surgical services.
Aims
This study aimed to identify and analyze the main impacts of the COVID-19 pandemic on surgical patient safety.
Methods
An integrative literature review was conducted using PubMed, SciELO, and the Virtual Health Library databases. The descriptors “COVID-19,” “general surgery,” and “patient safety” were applied according to MeSH terms, including studies in English, Portuguese, or Spanish from 2017 to 2021 that addressed the relationship between COVID-19 and patient safety in surgical settings. From 32 initially identified articles, 10 met the eligibility criteria and were included in the final analysis.
Results
COVID-19 is a highly contagious disease that can cause severe pulmonary involvement and was declared a pandemic by the World Health Organization in 2020, it profoundly affected healthcare systems, particularly surgical services. Elective procedures for benign conditions were initially postponed to reduce hospital burden and transmission risk, while emergency and oncologic surgeries were maintained. Safety strategies included preoperative testing up to 30 days before surgery, mandatory use of PPE, careful postoperative monitoring for pulmonary complications, and RT-PCR testing for symptomatic patients. Suspected or confirmed COVID-19 patients were managed in separate hospital circuits. Minimally invasive surgery, when performed with appropriate equipment and technique in asymptomatic patients, proved to be a valuable alternative, offering clinical benefits and potentially reducing viral transmission risk.
Conclusion
During the COVID-19 pandemic, strict adherence to PPE use, postoperative surveillance, and patient flow separation were essential to ensure surgical patient safety. The implementation of structured safety protocols and the appropriate use of minimally invasive techniques contributed to safer surgical care in a highly challenging epidemiological context.
Single-Port Endoscopic Nipple Sparing Bilateral Mastectomy in Male Gynecomastia: A Case Report
Abstract
Background
Gynecomastia is a condition of breast enlargement in men due to breast gland proliferation that is generally bilateral.
Conclusion
The case presents a 30-year-old man with bilateral gynecomastia, defined as painless, bilateral breast enlargement of glandular breast tissue without associated skin changes, nipple discharge, or palpable lumps. The diagnosis was confirmed by clinical and histopathological findings and treatment by single-port endoscopic nipple sparing bilateral mastectomy was uneventfully performed. This case highlights the significance of careful clinical examination and timely surgical treatment in patients with gynecomastia especially when the condition starts raising cosmetic or psychological issues with excellent results and fewer complications.
Case_presentation
A 30-year-old male presenting with bilateral breast enlargement noticed within the past month. There was no pain, no breast discharge, and no hard lump when palpated. On physical examination, there is symmetrical breast enlargement, without skin changes, nipple retraction, or any discharge. Glandular enlargement with a diameter of 5 cm, painless, immobile, firm borders, no galactorrhea, no palpable lumps. Laboratory examination was within normal limits. The diagnosis was bilateral gynecomastia. An endoscopic bilateral mastectomy was performed. Histopathologic findings supported the diagnosis of gynecomastia. The post operative course was unremarkable.
Extensive necrotic ileal intussusception in an adult with prior gastrectomy and metastatic gastric cancer: a rare surgical emergency
Abstract
Background
Adult intussusception is an uncommon cause of mechanical small bowel obstruction and is frequently associated with an underlying pathological lead point. Unlike paediatric cases, adult presentations are often non-specific, leading to delayed diagnosis and an increased risk of bowel ischaemia and necrosis. Early recognition using contrast-enhanced computed tomography (CT) is essential, as radiological findings guide urgent surgical management and influence operative strategy.
Conclusion
This case illustrates the critical role of contrast-enhanced CT in the early diagnosis of adult intussusception and in identifying radiological signs of bowel ischaemia and necrosis. Recognition of mesenteric involvement, reduced mural enhancement, and upstream dilatation should prompt urgent surgical intervention. Early imaging-driven decision-making is essential to prevent catastrophic complications and optimise outcomes in this rare life-threatening condition.
Case presentation
A 48-year-old woman with a history of total gastrectomy and partial oesophagectomy with Roux-en-Y reconstruction for gastric adenocarcinoma presented with acute abdominal pain and peritoneal signs. Contrast-enhanced CT demonstrated mechanical small bowel obstruction due to ileo-ileal intussusception involving the alimentary limb, with concomitant invagination of the adjacent mesentery. Marked signs of bowel compromise were present, including reduced mural enhancement, bowel wall thickening, and pelvic effusion. Arterial and venous mesenteric stenoses were identified, secondary to invagination, with associated features of digestive ischaemia. There was marked dilatation of the upstream alimentary and biliary limbs. Emergency surgical exploration confirmed extensive necrotic ileal intussusception of 60cm perforation of necrotic ileum with perforation of the jejunojejunostomy requiring resection of 100cm of common limb including the anastomosis leaving 3 bowel stumps. Given severe contamination and uncertain bowel viability, damage-control surgery with open abdomen management was performed. A planned second-look laparotomy at 30 hours confirmed bowel viability, allowing a new Roux-en-Y reconstruction with two small bowel anastomoses.



Preoperative Semaglutide Before Robotic Major Liver Resection in Obese patients– Preliminary Results
Abstract
Background
Obesity and hepatic steatosis are increasingly prevalent in hepatopancreatobiliary (HPB) surgery and are associated with prolonged operative time and higher morbidity. In minimally invasive major hepatectomy, these factors can further increase technical complexity. Pharmacological weight loss with GLP-1 receptor agonists may optimize surgical candidates, but data in major HPB surgery remain limited. Moreover, preliminary translational studies in rodents, support a potential role of GLP-1 in liver regeneration.
Aims
The aim of this pilot study, is to evaluate the impact of preoperative semaglutide (GLP-1) therapy on weight loss, hepatic steatosis, and perioperative outcomes in obese patients undergoing robotic major liver resection.
Methods
All consecutive high-BMI patients (median BMI 38 kg/m²) scheduled for robotic major liver resection between February and September 2025 received preoperative semaglutide for a median of 4 weeks. Endpoints included percentage weight loss, MRI-documented steatosis, perioperative outcome and feasibility.
Results
Ten patients were included and compliance with GLP-1 was >100%. Median preoperative weight loss was 7.2% (IQR 4.1–10%), corresponding to 11.4 kg. All patients showed signs of steatosis in MRI, with a major proportion of severe steatotic patients (n=6). After GLP-1 repeated MRI prior to surgery documented a descrease of steatosis in n=5/10 patients. n=7 patients underwent double vein embolization prior to hepatectomy and GLP-1 treatment was started after the intervention. Postinterventional GLP-1 treatment did not impair liver regeneration and completion hepatectomy could be performed in all patients. Indications included hepatocellular carcinoma (n=5), colorectal liver metastases (n=3), and cholangiocarcinoma (n=2). Overall, Robotic right hemihepatectomy was performed in n=8 patients, left hemihepatectomy in n=1, and parenchyma-sparing resection (≥3 Segments) in n=1. Only one patient experienced a major complication (Clavien–Dindo ≥IIIa).
Conclusion
Preoperative GLP-1 therapy is feasible, safe, and well tolerated in obese patients undergoing robotic major liver resection. It induces clinically relevant weight loss, reduces hepatic steatosis, and facilitates technically demanding procedures without impairing liver regeneration.
The Rare Case of a Sertoli Cell Tumor of the Adrenal Gland in a Man With Pathological Dexamethason Inhibition Test: A Case Report
Abstract
Background
Sertoli cell tumors are rare sex cord–stromal tumors accounting for approximately 1% of testicular neoplasms. Extragenital manifestations are extremely rare - only one case of a Sertoli cell tumor arising in the adrenal gland has been reported. We present the second known case of an adrenal Sertoli cell tumor in a male patient, presenting with a pathological dexamethasone suppression test.
Conclusion
Adrenal Sertoli cell tumors represent an extremely rare entity lacking specific management guidelines. In this case, robotic-assisted adrenalectomy proved safe and feasible. We saw a good short-term oncological and clinical outcome. Further reports are needed to clarify hormonal associations and establish standardized follow-up and treatment strategies.
Case presentation
An 82-year-old otherwise healthy man was referred for evaluation of an incidentally detected left adrenal mass. The patient was asymptomatic with no clinical signs of catecholamine excess, hypercortisolism, hyperaldosteronism or B-symptoms. Initial CT scan revealed a 44 × 42 mm lesion, which increased to 50 × 46 mm within three months and suspicious washout characteristics (Figure 1). Endocrinological work-up showed a pathological dexamethasone inhibition test, while metanephrines and aldosterone testing was normal. Tumor markers (AFP, β-HCG) were unremarkable. A hormonally active adrenal adenoma with autonomous cortisol production was suspected.
After discussion at the interdisciplinary tumor board, robotic-assisted adrenalectomy was performed (Figure 2). Complete resection was achieved without complications, the patient was discharged on the third postoperative day.
Histopathological examination showed a Sertoli cell tumor with complete excision and no evidence of local infiltration or malignancy (Figure 3).
Immunohistochemistry showed positivity for CD56, CD99, synaptophysin and partial positivity for SF1, calretinin and inhibin. Chromogranin A and MART1 were negative. Molecular analysis revealed no FOXL2 or DICER1 mutations. Postoperatively, hydrocortisone substitution was initiated due to submaximal cortisol response in ACTH stimulation testing. At six-month follow-up, CT imaging showed no recurrence or metastases and tumor markers remained normal.

Acute Idiopathic Gastric Necrosis Due to Gastric Dilatation: A Case Report
Abstract
Background
Acute gastric necrosis due to gastric dilatation is a rare but serious condition resulting from venous outflow obstruction. Traditionally associated with eating disorders, it is also described in patients with polytrauma and diabetes. Despite effective treatment, the mortality rate remains significant.
Conclusion
Acute gastric necrosis is a rare, potentially fatal condition requiring prompt diagnosis and intervention. Radical excision might be the safest approach due to the risk of complications from the poor healing of residual tissue. Employing a damage control strategy is advisable for patients in a shock, where anastomosis may pose significant risks during the initial procedure.
Case presentation
A 77-year-old man with a history of arterial hypertension, chronic alcohol use, gait disorders, and umbilical hernia repair, was admitted with acute left upper quadrant pain and repeated vomiting. Upon admission, vital signs where stable, but clinical exam revealed abdominal distension with peritoneal signs. An abdominal computed tomography scan (Figure 1) showed marked gastric distension, parietal pneumatosis and portal and mesenteric vein gas along with small bowel ileus, without signs of perforation. Additionally, a lesion in the right colonic’s flexure raised suspicion of a neoplasic lesion.
Initial management included nasogastric tube placement via gastroscopy. Exploratory laparoscopy revealed necrosis of the gastric greater curvature (Figure 2), confirmed by intraoperative gastroscopy, which showed transmural necrosis extending to the oesophagogastric junction. The patient’s condition deteriorated, leading to septic shock requiring significant adrenergic support. Following conversion to an open laparotomy, a total gastrectomy was performed, employing a damage control strategy that left the esophageal and duodenal stumps. After achieving hemodynamic stability, the planned second look procedure included eosophagojejunal anastomosis with Roux-en-Y reconstruction, feeding jejunostomy, cholecystectomy, and right hemicolectomy with ileo-colostomy for the suspected neoplasic lesion. Remarkably, the patient recovered without postoperative complications and was discharged to a rehabilitation program.


Spontaneous mesenteric hematoma following a sneezing episode associated with an intestinal pseudodiverticulum: a case report
Abstract
Background
Spontaneous mesenteric hematoma, historically referred to as abdominal apoplexy, is a rare and potentially life-threatening cause of acute abdominal pain. It is defined as bleeding into the mesentery in the absence of trauma or iatrogenic injury. Reported etiologies include anticoagulant therapy, vasculitides, connective tissue disorders, or pancreatitis; however, truly idiopathic cases remain exceptional. Diagnosis is challenging due to nonspecific clinical presentation and imaging findings that may mimic bowel ischemia or neoplasia
Conclusion
Spontaneous mesenteric hemorrhage can occur in otherwise healthy individuals and may be precipitated by transient increases in intra-abdominal pressure such as sneezing. Local structural abnormalities, including intestinal pseudodiverticula, may contribute to mesenteric vessel fragility and bleeding. Awareness of this rare entity may facilitate timely diagnosis and appropriate management.
Case presentation
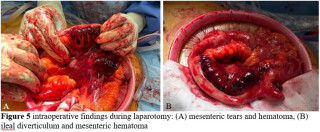
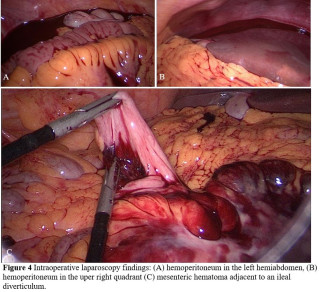
A 45-year-old man with no relevant past medical history presented with acute diffuse abdominal pain following a forceful sneezing episode. Physical examination revealed localized right-sided abdominal tenderness without peritoneal signs. Laboratory tests showed mild leukocytosis with normal inflammatory markers and hemoglobin. Contrast-enhanced computed tomography demonstrated a mesenteric hematoma associated with moderate hemoperitoneum and focal mural hypoenhancement of an ileal loop, without active arterial extravasation (Figure 1). Urgent surgical exploration revealed approximately 500 mL of hemoperitoneum, a large mesenteric hematoma, and an adjacent intestinal pseudodiverticulum (Figures 2-3). Segmental small bowel resection including the diverticulum was performed. Histopathological analysis confirmed fresh mesenteric hemorrhage and pseudodiverticular changes without evidence of malignancy, vasculitis, or vascular malformation. The postoperative course was uneventful, and the patient remained asymptomatic at six-week follow-up.
What to Expect When You Are Not Expecting: A Rare Case of Persistent Left Superior Vena Cava
Abstract
Background
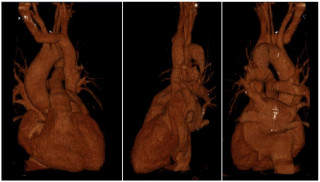
Persistent left superior vena cava (PLSVC) is a rare congenital vascular anomaly, resulting from the persistent patency of the left superior cardinal vein following early stages of venous system development. In most cases, PLSVC coexists along the right SVC and drains into the right atrium via the coronary sinus, without haemodynamic consequences. Usually asymptomatic, PLSVC is identified incidentally during imaging studies or invasive procedures, such as central venous catheterisation and pacemaker implantation. We present a case of an accidental PLSCV finding following a challenging catheterisation of the SVC during port placement.
Conclusion
This case report emphasises the critical importance of understanding central venous system anatomical variants. Identifying PLSVC can prevent complications and inform appropriate procedural strategies, particularly for venous catheterisation. Preprocedural imaging review, and eventually vascular consultation, are essential to identify such anomalies, ensuring safe and effective clinical outcomes.
Case presentation
A 57-years-old female was referred to general surgeons for port implantation before starting chemotherapy. Catheter insertion was planned on the right cephalic vein, but its progression proved impossible during the procedure. A right subclavian vein puncture was subsequently performed, allowing the guidewire to cross the right brachiocephalic vein and descend to left side of the heart. While suspecting incorrect placement, the right internal jugular vein was punctured under ultrasound control, yet the guidewire advanced laterally toward the left heart. Upon vascular consultation, images review of previously conducted scan revealed a patent PLSVC, which transversed posteriorly to the left atrium and drained into the right atrium through the coronary sinus. The right SVC was absent, replaced by a left brachiocephalic vein bridge that drained into the PLSVC (Figure 1). The catheter was placed into the PLSVC and the procedure completed (Figure 2). The patient developed a pneumothorax due to subclavian puncture, which was effectively managed by drainage placement, leading to an uneventful recovery.
Impact of Peer-Assisted Learning on Suturing Skill Acquisition in 194 Medical Students: A Multicenter Cohort Study
Abstract
Background
Developing foundational surgical skills is an essential element of medical education; however, a substantial proportion of medical graduates demonstrate limited proficiency or lack formal competence in
suturing.
Aims
This study investigated the effectiveness of peer-assisted learning on suturing skill progression and its influence on students’ engagement
with surgery.
Methods
Prospective study (2023–2025). Medical students in years 2–5 participated in three standardized 2-hour suturing sessions integrating e-learning with peer-assisted, supervised hands-on practice. Participants submitted video recordings of their suturing performance. Suturing videos were independently evaluated by surgeons from two different hospitals using the Objective Structured Assessment of Technical Skills (OSATS : 1-5 point), two-sided p value < 0.05 was considered statistically significant. Pre–post comparisons were assessed using paired
Results
A total of 194 enrolled medical students, completed the study; 161 participants were included in the final analysis. Mean performance increased by 0.95 points on the 5-point OSATS scale (p < 0.01). The largest gain was observed for procedural knowledge (“knowledge of steps”; mean increase 1.27, p < 0.01), whereas the smallest improvement was noted for tissue handling (mean increase 0.55, p < 0.01). Inter-rater reliability was moderat (IRR of 0.476) across four reviewers. Despite a very large
pre–post effect size (Cohen’s d = 4.01), inter-rater agreement on absolute OSATS scores was limited, with low correlations between reviewers (Pearson’s r = 0.067; Spearman’s ρ = 0.404), likely reflecting differences in
score calibration rather than inconsistency in observed skill. In multivariable analysis, skill progression was positively associated with higher perceived competence in suturing (β = 0.32; 95% CI [0.047, 0.55], p = 0.02)
Conclusion
Peer-assisted learning was associated with measurable improvements in basic suturing skills following the 6-hour suturing program.
Liver all Around- a Rare Case of Ectopic Gallbladder
Abstract
Background
Intrahepatic gallbladder (IHGB) is a rare congenital anomaly that occurs with a prevalence of 0.1%. It is associated with cholecystolithiasis, bile stasis, liver abscesses, bile duct carcinoma and can challenge diagnosis and surgery. We present a case in which IHGB was missed in preoperative ultrasound.
Conclusion
This case illustrates the challenge of preoperatively undiagnosed IHGB. Preoperative ultrasound may not reliably provide definitive evidence of aberrant GB position. In any doubt MRI or CT scan is recommended. Intraoperative ultrasound can be helpful. Be aware of associated liver anomalies that might complicate the procedure.
Case presentation
A 65-year-old woman presented to the outpatient clinic with severe right upper abdominal pain for two days, vomiting and diarrhea. Her medical history included mild renal insufficiency, cholecystolithiasis and atrial fibrillation treated with anticoagulants. Clinically, she presented with skin and scleral icterus and a positive Murphy's sign. Biochemical tests showed elevated inflammation and severe cholestasis parameters.Sonography revealed a gallbladder (GB) with multiple concrements, a thickened wall and dilated CHD (Figure 1). ERC with stenting was performed same day. She developed a mild post-ERC pancreatitis. Since on the fifth day after ERC inflammation markers remained elevated and ultrasound showed signs of inflammation cholecystectomy was indicated. Intraoperatively fibrinous peritonitis was observed in the right upper abdomen. An enlarged liver in non- anatomic position extended to the umbilicus. It was not possible to locate the GB so a laparotomy via Kocher incision was necessary. Even in open surgery the GB was untracable. The hepatic ligament with the palpable stent could be followed until the intrahepatic part. Intraoperative ultrasound located the completely intrahepatic GB (Figure 2). Dissection of the liver with diathermy allowed the inflamed GB to be removed. Histology showed only inflammation. The patient was discharged on the 11th postoperative day for further outpatient care.
From VATS to RATS: Extending Minimally Invasive Approaches to Advanced and Complex Lung Cancer Resections
Abstract
Background
Minimally invasive techniques have become central to the surgical management of non-small cell lung cancer (NSCLC). While video-assisted thoracoscopic surgery (VATS) is well established, robotic-assisted thoracic surgery (RATS) has emerged as a complementary platform with potential advantages in complex anatomical resections.
Aims
This study aims to report the impact of implementing a comprehensive RATS program in a high-volume single-center setting, focusing on the changes in surgical approach, perioperative outcomes, and the feasibility of minimally invasive surgery for complex cases.
Methods
Consecutive patients undergoing anatomical pulmonary resections for primary lung cancer or pulmonary metastases were analyzed across two periods: a pre-RATS era (two years prior to RATS introduction) and a RATS era (two years after implementation). Surgeons were experienced in VATS before transitioning to RATS. Cohorts were propensity-matched for age, sex, and oncological stage. Primary endpoints included surgical approach, perioperative outcomes, and feasibility of minimally invasive surgery in complex cases (post-induction therapy, sleeve resections).
Results
A total of 873 patients were included (pre-RATS: n=448; RATS era: n=425). Case mix and procedural distribution were comparable between groups. Following RATS implementation, the proportion of open resections significantly decreased (21.9% vs 12.7%, p<0.001), as did conversion rates (3.9% vs 3.0%, p=0.025). Minimally invasive surgery was increasingly feasible after induction therapy (31.7% vs 63.3%, p=0.005) and for sleeve lobectomies (18% vs 43%, p=0.011). Operative time and postoperative outcomes, including length of stay, drainage duration, and complication rates, were similar between groups.
Conclusion
Implementation of a RATS program in a high-volume center is safe and effective and is associated with reduced thoracotomy rates. Importantly, RATS facilitates the extension of minimally invasive approaches to more complex and locally advanced lung cancer resections, supporting its role in the modern multimodal treatment era.
Ulceroinfiltrative Lesion of the Distal Rectum Caused by a Probable Sexually Transmitted Infection
Abstract
Background
Sexually transmitted infections (STIs) with anorectal involvement have become increasingly prevalent and may clinically and endoscopically mimic inflammatory or neoplastic diseases. The absence of specific histopathological findings often delays diagnosis and management, reinforcing the importance of maintaining a high index of suspicion in patients with rectal lesions of unclear origin.
Conclusion
Rectal lesions of indeterminate etiology should raise suspicion of sexually transmitted infections, even when the causative pathogen cannot be clearly identified. Early recognition and appropriate investigation are essential for adequate management and for reducing disease transmission.
Case presentation
A 29-year-old male patient with no relevant medical history presented with diarrhea, abdominal pain, hematochezia, mucus in stools, and anal pain during defecation lasting ten days. Prior antiparasitic treatment was ineffective. Abdominal and pelvic computed tomography revealed mesorectal, obturator, and left iliac lymphadenopathy, rectal wall thickening, mesorectal fat stranding, and mild colonic distension. Colonoscopy showed an ulceroinfiltrative lesion in the distal rectum, 6 cm from the anal verge, occupying approximately 50% of the lumen, with poorly defined margins and fibrin deposits. Histopathological analysis demonstrated acute ulcerated proctitis without evidence of chronic inflammatory disease, granulomas, infection by fungi or parasites, or malignancy, suggesting a nonspecific infectious process. Empirical treatment with metronidazole was initiated, and pelvic magnetic resonance imaging and serological tests were requested. Follow-up colonoscopy demonstrated marked regression of the lesion, involving less than 10% of the rectal lumen, although mucosal friability persisted.
Haemorrhagic Shock Following Splenic Rupture Caused by an Infiltrative Metastatic Renal Tumour: A Rare Case Report
Abstract
Background
The most common cause of splenic rupture is trauma. Atraumatic aetiologies include hematologic malignancies or infections, whereas metastatic renal neoplasms represent an exceptional cause that has been rarely reported in the literature.
Conclusion
Our case report demonstrates an extraordinary case of per continuitatem infiltration of the spleen originating from a kidney tumour. This rare but clinically relevant complication should be considered as a differential diagnosis of splenic rupture especially in the absence of trauma.
Case presentation
A 72-year-old male patient presented with acute onset of thoracic and abdominal pain, additionally complaining of light-headedness and cold sweats. The medical history was unremarkable regarding previous trauma or infections, but the patients was recently diagnosed with a kidney mass. The patient was hypotensive, tachycardic, with cold peripheral extremities and tenderness in the epigastrium. Laboratory investigations showed mild anaemia and leucocytosis, impaired renal function, and high lactate. Ultrasonography suggested free fluid in the Morison’s pouch, a mass of the left kidney and inhomogeneous splenic tissue, confirmed by CT angiography, which revealed a hematoma of the spleen with signs of ongoing bleeding and free fluid in the abdominal cavity.
After initial stabilization with blood transfusions and phenylephrine, an endovascular approach was planned. However, the patient developed hypovolemic shock prior to the procedure, indicating urgent explorative laparotomy. After the splenic hilum was initially clamped, splenectomy was performed, resulting in hemodynamic stabilization. Subsequent exploration of the abdomen revealed peritoneal nodules and a tumour of the left kidney. Peritoneal biopsies were taken and showed a papillary renal cell carcinoma. The patient was referred for further diagnostic and treatment to the oncology department to receive chemotherapy.
The postoperative recovery was uneventful except for one additional blood transfusion and the patient was discharged on postoperative day six.

Transvaginal Small Bowel Evisceration 23 Years After Vaginal Hysterectomy
A Case Report
Abstract
Background
Transvaginal small bowel evisceration is an extremely rare but potentially life‑threatening surgical emergency, most commonly occurring after pelvic surgery. Delayed presentations several decades after hysterectomy are exceptional and pose diagnostic and therapeutic challenges. To report a rare case of transvaginal small bowel evisceration occurring 23 years after vaginal hysterectomy and to highlight the importance of interdisciplinary surgical management.
Conclusion
Transvaginal bowel evisceration can occur decades after hysterectomy. Prompt recognition and a structured interdisciplinary surgical strategy are essential to achieve favorable outcomes.
Case presentation
An 88‑year‑old woman presented with acute lower abdominal pain and transvaginal evisceration of approximately 50 cm of small bowel. She had undergone vaginal hysterectomy 23 years earlier for endometrial carcinoma in situ. Relevant comorbidities included metastatic melanoma and anticoagulation with rivaroxaban. The exposed bowel appeared livid but showed preserved peristalsis. Abdominal ultrasound revealed no free intra‑abdominal fluid or ileus.
An interdisciplinary open surgical approach involving general surgeons and gynecologists was chosen. A lower midline laparotomy was performed. The vaginal vault was enlarged, allowing reduction of the small bowel into the abdominal cavity with transvaginal assistance. The vaginal vault was closed transvaginally using a two‑layer suture, supplemented by unilateral right‑sided pectineal fixation. Abdominal wall closure was performed using a small‑bite technique.
The postoperative course was uneventful with no bleeding complications. Bowel function resumed on postoperative day four. The patient was discharged on postoperative day six. Transient urinary incontinence and mild fecal smearing were noted during follow‑up.



Paracolic Internal Hernia With Small Bowel Incarceration Without Surgical History: A Case Report
Abstract
Background
Internal hernias, including paraduodenal (the most common), pericecal, Foramen of Winslow, intersigmoid, and transmesenteric/transmesocolic hernias (the rarest), account for approximately 0.5–5% of all cases of intestinal obstruction. Owing to their rarity and nonspecific clinical presentation, they are frequently misdiagnosed, leading to significant morbidity.
Conclusion
Although rare, paracolic hernias should be considered in the differential diagnosis of small bowel obstruction in patients without prior abdominal surgery. High clinical suspicion, early diagnosis, and timely surgical intervention are essential for favorable outcomes.
Case presentation
An 82-year-old male presented to the emergency department with acute-onset lower abdominal pain and one episode of vomiting. His medical history was unremarkable, with no prior abdominal surgery. Laboratory tests revealed elevated lactate levels, while all other parameters were within normal limits. Abdominal computed tomography demonstrated a mechanical ileus with suspicion of an internal hernia.
Emergency diagnostic laparoscopy revealed partial herniation and incarceration of the small bowel through a paracolic defect. The procedure was converted to a mini-laparotomy, with mobilization of the ileocecal region, followed by segmental ileal resection approximately 1 meter proximal to the ileocecal junction, due to questionable bowel viability and a tight strangulation ring. The patient received intravenous antibiotic therapy, and oral intake was gradually reintroduced without complications. After satisfactory wound healing and decreasing inflammatory markers, secondary closure of the laparotomy wound was performed, followed by a rapid and uneventful postoperative recovery.

Staged Resection of a Giant Hypervascular Posterior Hemangioma with Foraminal Extension
Abstract
Background
Posterior mediastinal hemangiomas are rare and may mimic neurogenic tumors, particularly when associated with foraminal extension. Their hypervascularity and proximity to critical neurovascular structures make their surgical management challenging with no optimal operative approach to date.
Conclusion
Giant hemangiomas are rare. The suggested multidisciplinary staged approach was safe and resolved the patient’s symptoms.
Case presentation
Here we describe a multidisciplinary management of a superior sulcus, giant hypervascular, posterior mediastinal hemangioma with foraminal extension. A 69 year old female presented with progressive dyspnea and fatigue. CT-scan imaging revealed a superior sulcus, well circumscribed 9x9x5.5cm mass of the right posterosuperior mediastinum extending through the T1-T2 neuroforamen. Magnetic resonance imaging confirmed a dumbell invasion of the foramen with hyperintense T2 signal confirming its hypervascularization. A transthoracic core needle biopsy confirmed a cavernous hemangioma. Because of the progressive symptomatology, a surgical resection was decided. An initial embolisation of the hemangioma was performed by interventional radiology to reduce intraoperative bleeding. Then, the spinal surgeon proceeded with a T1-T2 posterior hemi-laminectomy to free the dura mater and the foramen from the tumor. The first rib and C7 nerve root were resected because involved in the tumor. The thoracic surgeon then performed a hemi-clamshell to dissect the subclavian vessels and the plexus which allowed en bloc resection of the tumor with the lamina and the first rib. The surgery was uneventful and the patient was discharged on postoperative day 8 with a complete resolution of the dyspnea and slight paresthesias in the C7 dermatoma.

The Appendix Strikes Back: An Exceptional Cause of Sepsis After Ileal Conduit Diversion
Abstract
Background
Radical cystoprostatectomy with Bricker ileal conduit diversion is an established treatment for severe, refractory radiation cystitis. Postoperative urinary sepsis is most commonly related to ascending infection, conduit obstruction, or anastomotic complications. Entero-urinary fistulas involving an ileal conduit are rare, and an appendiceal origin is exceptionally uncommon.
Conclusion
This case illustrates an extremely rare cause of recurrent urinary sepsis after ileal conduit diversion : an appendico-ileal conduit fistula. The presence of fecal material in the conduit should prompt urgent evaluation for an enteric fistula. Laparoscopic appendectomy with fistula closure can offer definitive treatment with excellent clinical outcomes.
Case presentation
A 70-year-old man with a history of prostate adenocarcinoma treated with pelvic radiotherapy underwent radical cystoprostatectomy with Bricker ileal conduit diversion for chronic radiation cystitis and persistent macrohematuria. The postoperative course was complicated by recurrent episodes of urinary sepsis. Two months after surgery, fecal material was observed in the ileal conduit, prompting surgical consultation. Cross-sectional imaging confirmed a fistulous communication between the appendix and the ileal conduit (Figure 1 & 2). The patient underwent laparoscopic appendectomy with direct closure of the fistulous tract. Recovery was uneventful, and the septic episodes resolved.
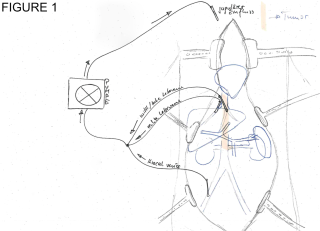
Total vascular exclusion of the liver with veno-venous ECMO in resection of a leiomyosarcoma of the inferior vena cava: A case report
Abstract
Background
Leiomyosarcoma is a rare malignant mesenchymal tumor originating from smooth muscle cells, characterized by aggressive growth and a high potential for metastasis.
Conclusion
Resection of an advanced leiomyosarcoma of the inferior vena cava is challenging but achievable. We employed a unique technique involving bypassing the liver and preserving right heart inflow, thus avoiding autotransplantation and its related complications.
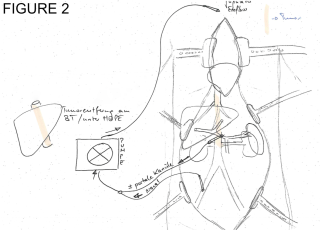
Case presentation
We report on a 76-year-old female who presented to the emergency department with increasing upper abdominal pain, a 2-month history of loss of appetite, and new bilateral leg edema. The diagnostic work-up revealed an intravascular tumor of the vena cava inferior extending from the right atrium to the right renal vein, measuring 15 cm in length. Biopsy confirmed the diagnosis of leiomyosarcoma. Upfront chemotherapy or radiation therapy was deemed inappropriate, and primary resection was planned.
As the primary surgical option, we planned to exclude the retrohepatic vena cava by preserving the hepatic inflow while connecting the liver veins to a v-v bypass to maintain cardiac inflow into the right atrium (Figure 1). Alternatively, a tumorectomy ex-situ on the backtable with in-situ bypass and auto-transplantation was our fall-back strategy.
The entire sarcoma was successfully removed without the need for auto-transplantation, including 20 cm of the inferior vena cava, which was reconstructed using bovine pericardium. Postoperatively, the patient stayed in the ICU for 2 days and was discharged to rehab after 12 days without any major complications.
Giant Intramuscular Hibernoma of the Thigh: Diagnostic Challenges and Surgical Treatment
Abstract
Background
Hibernoma is a rare benign lipomatous tumor originating from brown adipose tissue, accounting for less than 1% of benign adipocytic neoplasms. Fewer than 300 cases have been reported in the literature.
Due to its hypervascularity and heterogeneous appearance on imaging, it often mimics malignant neoplasms, such as atypical lipomatous tumors or liposarcomas, posing significant diagnostic challenges.
Conclusion
This case represents a rare brown adipose tissue tumor, known as hibernoma, located in the proximal thigh of a young patient. Surgical management is relatively straightforward; however, from a diagnostic standpoint, it is essential to exclude sarcoma, as MRI findings may appear similar. Immunohistochemical analysis and multidisciplinary discussion are therefore crucial before proceeding with surgical excision.
Case presentation
We report the case of a 37-year-old male presented with a slowly enlarging, painless mass of the anterior right thigh. Magnetic Resonance Imaging (MRI) identified a well-circumscribed, deeply seated intramuscular lesion within the quadriceps femoris, measuring 16x15x5 cm, exhibiting heterogeneous signal intensity and prominent internal vascularity. A core needle biopsy demonstrated a lipomatous neoplasm composed of brown fat–like cells with focal spindle cell and myxoid features. Molecular analysis showed absence of MDM2 amplification, supporting a benign diagnosis. Following a multidisciplinary consultation, a complete surgical excision of the mass, weighing approximately one kilogram, was performed.
Macroscopically, the tumor was well-encapsulated and easily cleaved from the surrounding muscle fibers without evidence of local infiltration (figure 1, figure 2). Final histopathological examination confirmed the diagnosis of intramuscular hibernoma without evidence of malignancy (figure 3). Patient was discarged on post-operative day two in good general conditions. The postoperative course was uneventful, with preserved limb function and no complications.

Radial dislocation of the median nerve after volar plate fixation of a distal radius fracture: a case report
Abstract
Background
Median nerve neuropathy and secondary carpal tunnel syndrome are well-recognized complications following volar plate fixation of distal radius fractures. In contrast, late-onset anatomical displacement of the median nerve has rarely been described.
Conclusion
This case highlights a rare but clinically relevant cause of late-onset median nerve neuropathy after volar plate fixation of a distal radius fracture. Persistent or atypical neurological symptoms long after fracture healing should prompt consideration of structural nerve pathology. In this context, removal of osteosynthesis material should be regarded as revision surgery, as unexpected nerve displacement may be encountered and requires meticulous surgical technique.
Case presentation
We present the case of a patient who developed persistent wrist pain and sensory disturbances involving all digits approximately one year after volar plate fixation of a distal intra-articular radius fracture. Clinical and electrophysiological evaluations were consistent with secondary carpal tunnel syndrome, with additional evidence of ulnar nerve involvement at Guyon’s canal. Due to persistent symptoms, revision surgery including osteosynthesis material removal was performed. Intraoperatively, the median nerve was found to be markedly dislocated in a radial direction, following an abnormal curved course and lying superficially beneath the radial subcutaneous tissue. Focal compression was identified at the level of the carpal tunnel inlet between the flexor pollicis longus and flexor carpi radialis tendons. Microsurgical neurolysis, decompression of the carpal tunnel and Guyon’s canal, and medial repositioning of the median nerve were performed.
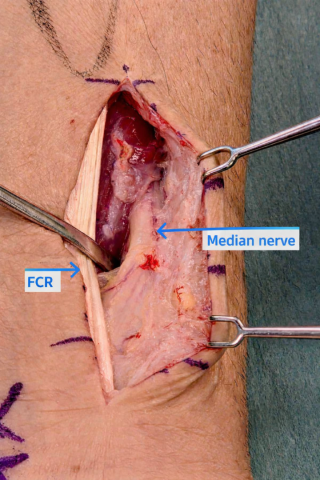
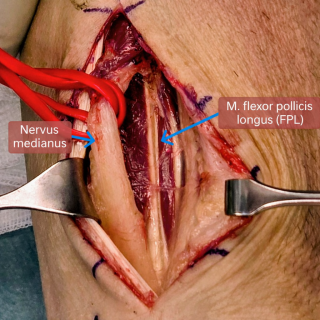

Feasibility of ICG Fluorescence for Intraoperative Imaging of Non-CRLM and Non-HCC lesions – A Case Series
Abstract
Background
Indocyanine green (ICG) fluorescence imaging for the intraoperative visualization of hepatocellular carcinoma (HCC) and colorectal liver metastases (CRLM) has been widely reported in the literature. Its role in highlighting other liver lesions remains insufficiently characterized, with existing evidence limited to heterogeneous series and isolated reports. Several non-colorectal malignancies, including breast cancer and gastrointestinal stromal tumor (GIST) metastases, as well as benign lesions such as focal nodular hyperplasia, have been reported to exhibit variable fluorescence behavior.
Aims
To evaluate the feasibility and histology-specific intraoperative fluorescence behavior of ICG in non-HCC, non-CRLM operated in our institution.
Methods
We retrospectively analyzed a case series of patients undergoing liver resection for non-HCC and non-CLRM from May 2024 to August 2025. ICG was administered intravenously between 24-48h preoperatively, using a dosage of 0.5mg/kg. Intraoperative near-infrared fluorescence imaging was performed in combination with intraoperative ultrasound. Fluorescence findings were recorded and correlated with final histopathological diagnosis.
Results
A total of eleven patients were included. Pathologies comprised breast cancer liver metastases, GIST metastases, neuroendocrine tumor (NET) metastases, and benign lesions including adenomas. Positive intraoperative fluorescence was observed in breast cancer metastases (Fig.1), GIST metastases, focal nodular hyperplasia (Fig.2) and adenomas (Fig.3), facilitating lesion localization during surgery. In contrast, the two neuroendocrine tumor metastasis cases did not demonstrate fluorescence in this series.
Conclusion
ICG fluorescence imaging appears to be a feasible adjunct for intraoperative visualization of other less explored liver lesions, including breast cancer and GIST metastases. Fluorescence behavior is dependent on several factors, including histology, administration techniques and patient characteristics influencing biliary excretion. The absence of uptake in NET metastases in our case series contrasts to what reported in the literature, highlighting biological variability and potential limitations of the technique. These findings support the need for larger, standardized and histology-specific studies to better define the role of ICG fluorescence beyond CRLM and HCC resections.
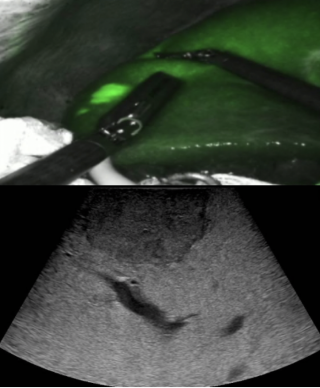
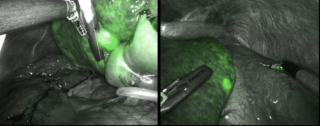

Beyond the Groin: Internal and Transthoracic Littre’s Hernias – A Rare Case Series Surgeons Should Be Aware of
Abstract
Background
A Littré’s hernia is defined by the presence of a Meckel’s diverticulum within a hernia sac and is classically described in inguinal, femoral, or umbilical hernias. Internal and transthoracic Littré’s hernias are exceptionally rare and remain poorly characterized, often leading to delayed diagnosis. To our knowledge, this case series is the first to describe exceptionally rare locations of Littré’s hernia.
Aims
It aims to raise awareness among surgeons of this uncommon and specific entity, which is notoriously difficult to diagnose preoperatively.
Methods
We report a case series of seven patients with internal or transthoracic Littré’s hernias identified in literature. Research was conducted on Pubmed database in order to analyze clinical presentation, imaging findings, anatomical location, surgical management and outcomes.
Results
Seven cases were identified (six men, one woman). Hernia locations were intra-abdominal in five cases (foramen of Winslow, transmesocolic, transomental) and transthoracic through acquired diaphragmatic defects in two cases. Clinical presentation varied according to location: transthoracic cases presented with respiratory and abdominal symptoms, whereas intra-abdominal cases presented with bowel obstruction features. Computed tomography (CT) identified internal herniation but failed to diagnose Meckel’s diverticulum in all cases. Four procedures were initiated laparoscopically, all requiring conversion to laparotomy. Resection of the Meckel’s diverticulum was performed in all patients, with additional bowel resection when indicated. Among transthoracic Littré’s hernias, one patient recovered without complications, while the other died on postoperative day 111 from hospital-acquired pneumonia. For abdominal Littré’s hernias, a single postoperative death was reported in 1968.
Conclusion
Internal and transthoracic Littré’s hernias are rare and potentially life-threatening entities with misleading clinical presentations. Awareness of these atypical locations and presentations is essential to avoid diagnostic delay. Early surgical intervention with systematic inspection of the small bowel, even in the absence of specific CT findings, and resection of the Meckel’s diverticulum remains the cornerstone of management.
Dysfunctional Jejunojejunostomy After Roux-en-Y Gastric Bypass
Abstract
Background
Persistent abdominal pain after Roux-en-Y gastric bypass (RYGB) remains a diagnostic and therapeutic challenge. Up to one third of patients report chronic postoperative abdominal symptoms. Standard imaging frequently fails to identify an anatomical pathology.
Growing evidence suggests that dysfunction of the jejunojejunostomy (JJ) represents an underestimated cause of postprandial pain, nausea and functional impairment. Patients are therefore misattributed to psychosomatic disorders.
Our aim is to illustrate JJ dysfunction as a clinically relevant and underdiagnosed cause of refractory postprandial pain after RYGB. We demonstrate the diagnostic and therapeutic value of surgical revision.
Conclusion
JJ dysfunction is an underestimated cause of persistent postprandial pain after RYGB. When non-invasive diagnostics are inconclusive, early surgical exploration and JJ revision should be considered.
Case presentation
We report the case of a 41-year-old woman with RYGB surgery (2015) and multiple abdominal revisions who developed new-onset, severe postprandial left-sided abdominal pain after robotic repair of a trocar hernia in December 2024. All previous bariatric revisions included closure of the mesenteric defects. Extensive diagnostic workup with repeated CT imaging (Picture 1), gastroscopy, colonoscopy and enteroscopy failed to demonstrate obstructive pathology. A radiopaque intraluminal structure was intermittently visualized in the jejunum but not confirmed endoscopically.
Ongoing symptoms caused inability to work and significant quality-of-life impairment. Therefore, we performed a diagnostic laparoscopy and a revision of the JJ.
Intraoperatively, the JJ was found to be severely pathological, showing extensive adhesions, fibrotic remodeling, an elongated rigid anastomosis with a long blind limb and mechanical distortion consistent with functional obstruction (Pictures 2, 3). Resection of the dysfunctional JJ with complete reconstruction of the alimentary and biliopancreatic limbs and closure of mesenteric defects was performed via mini-laparotomy.
The patient experienced rapid and sustained resolution of postprandial pain with full functional recovery.
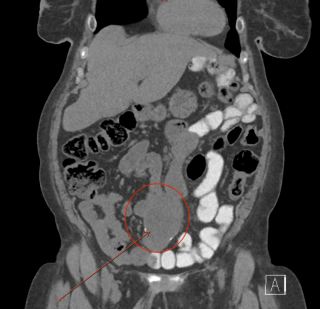
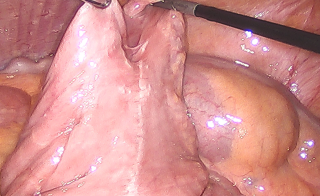
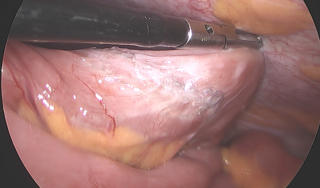
Diagnostic Pitfall of Para-Duodenal Paragangliomas: A Case Report and Implications for Perioperative Management
Abstract
Background
Paragangliomas are rare extra-adrenal neuroendocrine tumors that may occur in atypical abdominal locations. When arising in the para-duodenal region, they can closely mimic gastrointestinal stromal tumors (GISTs) or non-functioning neuroendocrine tumors (NETs). Failure to recognize this entity preoperatively may result in omission of mandatory biochemical testing and expose patients to significant perioperative risk.
Aims
To highlight a diagnostic pitfall of para-duodenal masses with important implications for perioperative safety and surgical management.
Methods
We present the case of a 71-year-old woman in whom a para-duodenal mass was incidentally detected during abdominal imaging. MRI and endoscopic ultrasound with fine- needle biopsy suggested a non-functioning NET or GIST arising from the muscularis propria. Due to the atypical location and absence of catecholamine-related symptoms, paraganglioma was not suspected, and no preoperative biochemical testing for metanephrines was performed. The patient underwent elective laparoscopic resection.
Results
Intraoperatively, a well-encapsulated mass was identified adjacent to—but not originating from—the duodenum and was completely excised laparoscopically without complications. Histopathological examination revealed a paraganglioma with classic Zellballen architecture and S-100–positive sustentacular cells (Figs. 1 and 2) . Immunohistochemistry showed preserved SDHB/SDHA expression and a low proliferative index (Ki-67 < 2%). Postoperative plasma-free metanephrines were within normal limits, confirming a non-functional tumor. The postoperative course was uneventful, and no recurrence was detected at short-term follow-up.
Conclusion
Para-duodenal paragangliomas are a rare but clinically relevant diagnostic pitfall for surgeons. Even in asymptomatic patients, they should be included in the differential diagnosis of para-duodenal masses with neuroendocrine features. In accordance with Endocrine Society and ESE/ENSAT guidelines, preoperative biochemical testing is essential to ensure perioperative safety and optimal surgical management
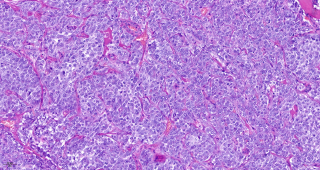
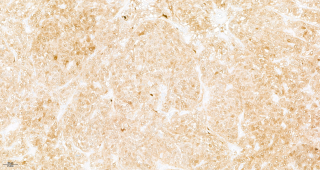
Symptomatic Intraperitoneal mass : Lipoma or liposarcoma ?
Abstract
Background
Lipomas are the most common benign mesenchymal tumors. Intra-abdominal localizations are rare and usually incidentalomas, with symptoms mainly related to mass effect when present[1].
Conclusion
Intra-abdominal lipomas are rare and may mimic malignant lipomatous tumors. Surgical resection is justified in symptomatic patients or when malignancy cannot be confidently excluded despite biopsy and molecular analysis.
Case presentation
We report the case of a 79-year-old woman with metabolic syndrome presenting with several months of abdominal pain, diarrhea, and abdominal distension. CT revealed an intraperitoneal para-colonic mass. MRI showed a well-circumscribed, predominantly fatty lesion attached to the mid-ascending colon, measuring 8x6.5x9 cm, suspicious for liposarcoma. Colonoscopy showed no intraluminal lesion or extrinsic compression (Figure 1). Percutaneous biopsy (Figure 2) demonstrated steatonecrosis with inflammatory fibrous remodeling, no MDM2 amplification on FISH. Following multidisciplinary sarcoma board discussion, laparoscopic resection (Figure 3) was performed (PCI score 0). Histopathology confirmed a benign lipoma, and postoperative recovery was uneventful.
Giant intra-abdominal or para-colonic lipomas are rare, predominantly affecting elderly women. They are most frequently located in the ascending colon (52%), usually small and asymptomatic[2]. However, some lesions may reach large sizes, up to 7x29x24 cm, and become symptomatic. Clinical presentation is variable and mainly related to compression, ranging from abdominal pain and bowel habit changes to rarer complications such as intussusception[3, 4].
Their true incidence remains unknown, as many cases are asymptomatic. Post-mortem studies report an incidence between 0.32%-to-4.4%. The main diagnostic issue is differentiation from malignant lipomatous tumors, particularly liposarcomas[1].
CT and MRI are essential for lesion characterization. Liposarcomas are generally larger (>10 cm) and present thick septa (>2 mm), non-adipose components, and heterogeneous features, but imaging alone may be insufficient to exclude malignancy[5].
Histological confirmation is therefore required. MDM2 gene amplification assessed by FISH reliably distinguishes liposarcomas from benign lipomas. Surgical resection is indicated in suspected malignancy symptomatic mass effect[6].
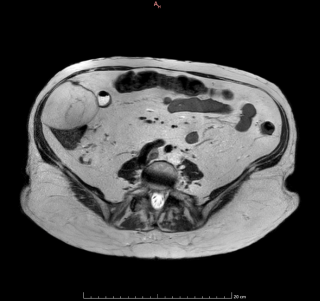
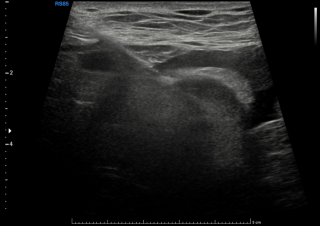
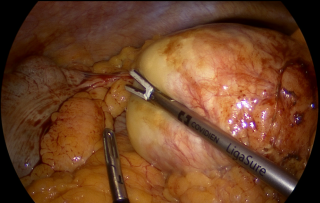
Impact of Preoperative Obstructive and Infectious Complications on Liver Fibrosis in Choledochal Cysts
Abstract
Background
Patients with choledochal cysts (CC) may present with associated complications, most commonly infectious or obstructive. Further, intraoperative liver biopsies often reveal hepatic fibrosis, indicating associated liver injury.
Aims
This study aimed to determine whether infectious and/or obstructive complications occurring before surgical management for CC were associated with an increased prevalence of liver fibrosis.
Methods
Retrospective review of children aged 0-16 years who had undergone surgical management for CC in our center, from 01.01.2009 to 31.12.2025. Obstructive complications were defined as cholestasis, cholelithiasis, pancreatitis; infectious events as cholecystitis, cholangitis, biliary peritonitis. Intraoperative liver biopsy specimens were assessed for fibrosis using the METAVIR scoring system. Patient exclusion: liver biopsy unavailable or insufficient for assessment. Clinical and pathological data were analysed descriptively with quantitative variables presented as medians (range) and qualitative variables as frequencies and percentages. Group comparisons were performed using Fisher’s exact test.
Results
Thirty-five patients underwent surgical treatment for CC, of whom 29 met the inclusion criteria. For the 24 postnatally diagnosed patients median age at diagnosis was 2 years (range: 0.17–15 years), 5 patients were diagnosed prenatally. 27/29 patients had Todani type I CC, 1 type II and 1 type IV. Eighteen patients experienced obstructive complications, 5 infectious and 3 experienced both. Hepatic fibrosis was more frequently observed in patients who had experienced both obstructive and infectious events (67%), than in those with obstructive or infectious events alone (33% and 0%, respectively) (all p > 0.35). Patients with no preoperative events had 11% fibrosis (Figure 1). None of the prenatally diagnosed patients showed liver fibrosis.
Conclusion
Preoperative obstructive complications, especially when combined with infectious events, are associated with a higher prevalence of hepatic fibrosis in CC patients. These findings highlight the importance of early detection and prompt surgical management of CC patients to mitigate the risk of liver fibrosis.
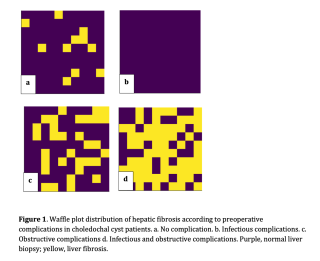
Varico–Portal Bypass with Superficial Femoral Vein for Chronic Superior Mesenteric Vein Thrombosis and Portal Hypertension with Colonic Variceal Bleeding
Abstract
Background
Surgical shunt procedures for variceal bleeding secondary to portal hypertension are currently rarely performed because of advances in medical therapy and the widespread use of interventional radiology and endoscopic techniques. However, surgery may remain necessary in complex cases.
Conclusion
Varico-portal bypass using superficial femoral vein may represent a safe and effective option to treat complicated portal hypertension safely.
Case presentation
A 32-year-old man with extensive superior mesenteric vein thrombosis of multifactorial origin (previous sleeve gastrectomy, pancreatitis, and antiphospholipid antibody syndrome) presented with recurrent lower gastrointestinal bleeding while receiving oral anticoagulation. Diagnostic workup demonstrated severe portal hypertension with extensive splanchnic involvement and active bleeding from right colonic varices. As thrombosis extended into peripheral venous branches, an interventional radiology approach was not feasible, and laparotomic surgical decompression was indicated after multidisciplinary discussion. After imaging review, three potential shunts were identified: varico-splenic at the pancreatic body, varico-external right iliac, or a portal bypass. Intraoperatively, the main varix draining the right colon was identified. A varico-splenic shunt was excluded because of excessive distance between vessels and extensive peripancreatic collateral circulation; therefore, a varico-portal venous bypass was planned. The left superficial femoral vein was harvested as an autologous graft, preserving the great saphenous and profunda femoris veins. An end-to-side anastomosis between the conduit and the portal vein was created, followed by antepancreatic retrogastric conduit positioning and an end-to-side anastomosis to the colic varix.
Immediate decompression of all splanchnic variceal circulation was observed. The postoperative course was uneventful. At one-year follow-up, no further episodes of hematochezia or rectal bleeding occurred despite full-dose anticoagulation. Colonoscopy at six months showed absence of red spots. Bypass patency was confirmed by Doppler ultrasound and contrast-enhanced magnetic resonance imaging.
Peculiar Pulmonary Mass
Abstract
Background
Pneumocytomas, first described by Liebow and Hubbell in 1956, are rare, mostly benign tumors, although cases with malignant transformations are described. They are more frequent in women of eastern Asian descent, with a higher incidence in middle age. They typically present as asymptomatic, incidental findings of solitary peripheral mass in the lower lobes. They present a unique surgical challenge due to their rarity and lack of consensus regarding management.
Conclusion
Treatment of choice for pneumocytomas is surgical resection, preferably sublobar, if adequate resection margin can be achieved, with usually excellent prognosis. Although the guidelines for pneumocytoma are non-existent, a follow up is needed due to the possibility of lymph node spread and local recurrence.
Case presentation
50-yo, otherwise healthy, nonsmoker female patient had an abdomen-CT scan due to intermittent epigastric pain, which revealed a 6cm, well delineated tumor in left lower lobe as an incidental finding. A chest-CT scan was also obtained, revealing no signs of mediastinal lymphadenopathy or other pathological lesions. The lung function tests were normal. The case was presented to an interdisciplinary tumorboard, and resection was recommended. We chose the open thoracotomy and fissureless approach due to the size of the tumor, thick adhesions and subtotaly fused interlobar fissure. During the dissection of the infracarinal lymph nodes to facilitate the bronchial division, a part of n. vagus had to be removed. During the postoperative course there was mild air leak which resolved spontaneously, the drainage could be removed on postop day 4. The patient suffered from nausea and disrupted gastrointestinal motility, which we managed with metoclopramide. The patient was discharged on postop day 7. The pathology revealed a 58 mm pneumocytoma, presenting with sclerotic, solid growing tumor-cell clusters with no mitotic figures, positivity for EMA and TTF1 as well for pancytokeratin superficially and low Ki-67 proliferation index.
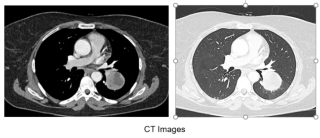
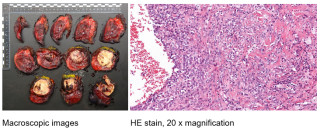
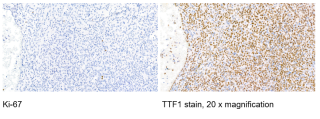
A Rare Case of Gallbladder Volvulus: The Hidden Twist
Abstract
Background
Gallbladder volvulus is a rare but serious surgical condition caused by the twisting of the gallbladder around its mesentery, leading to vascular compromise. It occurs in approximately 1 in 350’000 hospital admissions and predominantly affects elderly women. Arising from congenital or acquired anomalies of the gallbladder mesentery, it is often associated with loss of supporting tissue, increased peristaltic activity, or gallbladder verticalization due to kyphoscoliosis. Clinical presentation is nonspecific, frequently mimicking acute cholecystitis, which explains why fewer than 10% of cases are diagnosed preoperatively. Because of the risk of necrosis and perforation, early recognition and prompt surgical intervention are crucial. This case report aims to describe a case of gallbladder volvulus and present a brief review of the literature.
Conclusion
Gallbladder volvulus remains a diagnostic and therapeutic challenge due to its rarity and nonspecific presentation. Imaging, particularly MRI, may reveal a distended and malpositioned gallbladder, but diagnosis is often intraoperative. Emergency cholecystectomy is the treatment of choice, as conservative management is ineffective. This case highlights the importance of maintaining a high index of suspicion, particularly in elderly women or patients not responding to conservative measures, to improve outcomes in this rare but potentially fatal condition.
Case presentation
An 87-year-old woman with a history of hiatal hernia presented with acute epigastric pain lasting one day. Physical examination revealed a periumbilical palpable mass. CT imaging (Figures 1-2) showed marked gallbladder distension with cholelithiasis and features suggestive of cholecystitis. Laparoscopic cholecystectomy was performed on the same day.
Intraoperative exploration (Figure 3) revealed a 360° torsion of the gallbladder located in the right iliac fossa, with areas of necrosis but no perforation. The volvulus was reduced, and a standard cholecystectomy with critical view of safety was performed. The postoperative course was uneventful, and the patient was discharged the next day. Histopathological analysis confirmed the diagnosis.
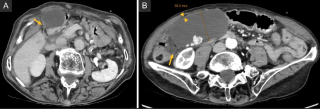
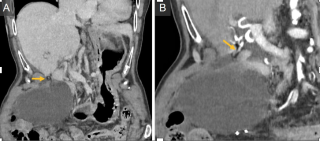
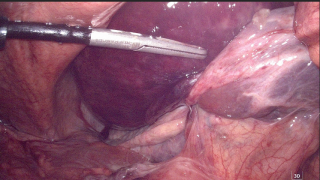
Pessary-Induced Rectovaginal Fistula in Advanced Prolapse : Successful Repair Using Transvaginal Approach Without Fecal Diversion.
Abstract
Background
Rectovaginal fistulas are uncommon but disabling. In developed countries, the etiology is predominantly iatrogenic injury, obstetric trauma, perianal abscess, Crohn's disease, malignancy, and radiation. Pessary-induced fistulas represent a rare complication, with a reported prevalence of less than 1% in routine care, increasing to 3% in patients with risk factors such as advanced pelvic prolapse, prior pelvic surgery, and advanced age. The underlying pathophysiology involves tissue ischemia and necrosis caused by prolonged pessary contact, particularly in the setting of advanced prolapse. Standard surgical treatment includes rectal submucosal advancement flap repair via an endorectal approach or vaginal flap via a transvaginal approach.
Conclusion
This case illustrates successful management of a pessary-induced anovaginal fistula using a predominantly transvaginal approach without fecal diversion. This technique offers the advantage of operating through a low-pressure compartment, reducing mechanical stress and facilitating healing.
Case presentation
We report the case of an 80-year-old woman (G3P2) with stage IV vaginal vault prolapse who had previously undergone vaginal hysterectomy and both posterior and anterior colporrhaphy. In early 2025, she was managed with a pessary for recurrent prolapse and developed vaginal brownish discharge and recurrent urinary tract infections after three months of pessary use. Clinical examination revealed a low rectovaginal fistula located 3.5 cm from the anal verge, above the anal sphincter complex, with preserved sphincter function. Colonoscopy and pelvic MRI confirmed the fistula without evidence of abscess, malignant features or underlying inflammatory disease. She underwent combined Richter’s sacrospinofixation with rectal submucosal advancement flap repair via transvaginal approach, using multilayer offset paletot sutures. The rectal mucosa was closed by simple sutures. No fecal diversion was performed. Postoperative follow-up demonstrated complete fistula healing. Although vaginal vault prolapse recurred on later follow-up, repeated clinical examination confirmed fistula closure at 6 months.
The Non-Recurrent Inferior Laryngeal Nerve, an Unexpected Guest During Thyroidectomy: About two Cases
Abstract
Background
The recurrent laryngeal nerve is a branch of the vagus nerve (VN) providing motor and sensitive function to the larynx. It usually describes a loop as it turns upward, passing under the subclavian artery on the right and recurring around the ligamentum arteriosum on the left. A nonrecurrent laryngeal nerve (NRLN) is a rare anatomical variation in which the nerve enters the larynx directly from the cervical VN. It has been reported in 0.3-0.8% of the population. The NRLN is closely related to the occurrence of rare vascular anomalies, such as arteria lusoria. Damage to this nerve during the surgical procedure may lead to severe morbidity.
Conclusion
The non-recurrent laryngeal nerve is a rare but significant anatomical variation that can turn a routine thyroidectomy into an unexpected challenge. While IONM is a valuable tool, the prevention of nerve injury ultimately relies on the surgeon’s patience, careful dissection, and systematic attention to anatomical landmarks. Vigilance and anticipation remain the most reliable safeguards against this “unexpected guest.”
Case presentation
Case 1: A 71-year-old woman was admitted for the management of a multi-nodular goitre. The preoperative contrast-enhanced computed tomography (CT) showed no vascular abnormality (figure 1). The team proceeded to total thyroidectomy with routine identification of the inferior laryngeal nerve and systematic use of intraoperative neuromonitoring (IONM). On the right side, the lower laryngeal nerve had not been identified on its usual path; it came directly from the VN and was heading towards the right tracheal cricothyroid angle (figure 1).
Case 2: A 54-year-old man was admitted for the management of a multi-nodular goitre. The preoperative CT showed an arteria lusoria as a vascular anatomic variation (figure 2). The surgery confirmed a NRLN on the right side (figure 3). No loss of signal was noticed.
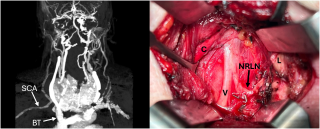
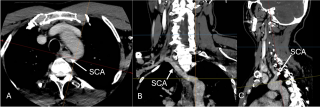
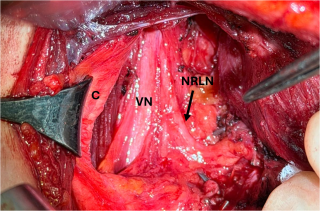
Colonic Intussusception due to an Undifferentiated Spindle Cell Sarcoma With Partial Smooth Muscle Differentiation: A Case Report
Abstract
Background
Intestinal intussusception is predominantly a paediatric condition, with most cases arising from benign causes. In contrast, adult intussusception is a rare event, accounting for approximately 5% of all cases with differences in its presentation, its management and—most notably—in its etiology. Intussusception occurs predominately in the small bowel, followed by the colon in approximately 20% of cases. More than 50% of all adult cases are related to a malignant process. This is particularly true in colo-colonic intussusception, where approximately 70% of cases are caused by malignancy, most commonly adenocarcinoma, lymphoma, and metastatic carcinoma.
Conclusion
Among the different sites of intussusception, colonic involvement is associated with the highest risk of malignancy and has even been identified as a significant predictive factor for malignancy. Nevertheless, sarcoma remains an exceptionally rare malignant cause of colo-colonic intussusception, accounting for only 0.015% of cases in a 2025 systematic review of 37 studies. Given the aforementioned risk of malignancy, surgical management should favor an en bloc resection without prior reduction to ensure oncological safety.
Case presentation
We report the case of an 87-year-old patient with a history of mid-rectal adenocarcinoma treated by low anterior resection in 2004 and adjuvant radio-chemotherapy, whose last colonoscopy in 2014 showed no abnormalities. She presented to the emergency department with intermittent abdominal pain evolving over several days, associated with two episodes of hematochezia. Abdominal CT scan revealed a right-sided colo-colonic intussusception with a mass effect, suggestive of an underlying malignant lesion. An urgent exploratory laparotomy with a right hemicolectomy was performed without prior reduction of the intussusception. Histopathological examination identified an undifferentiated ulcerated spindle cell sarcoma with partial smooth muscle differentiation, pT1, pN0, R0. Following a multidisciplinary team discussion, no adjuvant treatment was recommended. A long-term surveillance for pulmonary metastases is to be carried out under the supervision of the primary care physician.
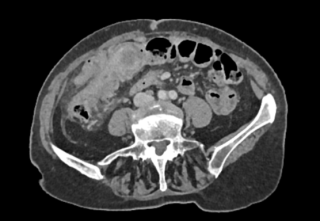

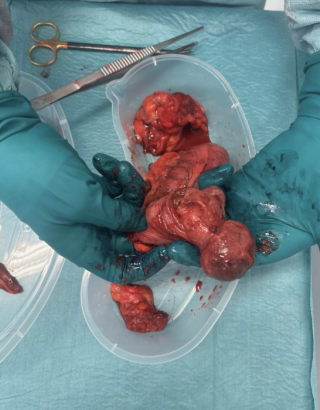
Neoadjuvant Immunotherapy for Resectable Colon Cancer Outside Clinical Trials: Lessons from a Swiss Real-World Cohort
Abstract
Background
Neoadjuvant immunotherapy has shown promising results in patients with mismatch repair deficient (dMMR) colon cancer under controlled trial conditions. The NICHE-2-Trial reported high response rates and limited toxicity. However, real-world data of routine clinical practice remain scarce. We report our experience with Checkpoint-Inhibitors (ICIs) for resectable colon cancer (cT3-cT4, N0/N+) outside of clinical trials.
Aims
Primary endpoints were immune-related adverse events and impact on surgical timing. Secondary endpoints included pathological response, N-status, surgical outcomes and early oncological follow-up.
Methods
All consecutive patients with resectable, non-metastatic dMMR colon cancer treated with ICIs at a tertiary referral center were retrospectively analyzed. Treatment regimens were adapted from published trial protocols. Only when insurance coverage was refused, Pembrolizumab was used instead of Ipilimumab and Nivolumab.
Results
Between 01/2023 and 01/2026 16 patients received ICIs in neoadjuvant setting. Immune-related adverse events occurred in 6 patients, 3 classifying as severe. One patient was no longer operable due to immunotherapy-related myositis, myocarditis and hepatitis, while in another a pembrolizumab-related duodenitis and gastric ulcera caused therapy suspension. Standard oncological resection with adequate lymphadenectomy was achieved in all operated patients (n=12). A complete pathological response was observed in 5 patients. In one case despite complete regression of the primary tumor, a vital metastatic lymph node was reported. No postoperative complications occurred. In median follow-up of 15 months no recurrences and one non-treatment-related death were observed.
Conclusion
In routine clinical practice, neoadjuvant immunotherapy for resectable dMMR colon cancer may be associated with significant immune-related toxicity, impacting surgical timing and feasibility. Although tumor regression rates are high, a subset of patients does not achieve pathological regression, underscoring the need for reliable predictive biomarkers to identify non-responders prior to treatment initiation. Therefore, careful patient selection and close interdisciplinary monitoring are essential. In this context, establishment of a national registry would be beneficial.
Biliopancreatic Limb Obstruction Caused by Intraluminal Bleeding of the Excluded Stomach After Roux-en-Y Gastric Bypass
Abstract
Background
Early bleeding after Roux-en-Y gastric bypass (RYGB) is a rare complication (0.9% to 4.4%), typically occurring in the postoperative period (mostly within 72 hours). Most bleeding events originate from anastomotic or staple-line sites (gastrojejunal 56%, jejunojejunal 11%), while the excluded stomach is an unusual source. In exceptional cases, bleeding may result in intraluminal clot formation, leading to bowel obstruction. We present a case of excluded stomach bleeding complicated by biliopancreatic limb obstruction after RYGB.
Conclusion
This case highlights a rare sequence of events following early a postoperative bleeding after RYGB, originating from the excluded stomach and leading to intraluminal clot formation with secondary biliopancreatic limb obstruction and staple-line dehiscence. In patients presenting early after RYGB with abdominal pain, anemia, and radiological signs of bowel dilation, intraluminal clot obstruction should be considered. Prompt diagnosis and surgical management are essential to limit morbidity.
Case presentation
A 40-year-old woman presented to the emergency department, two days after a RYGB for class II obesity, with acute left upper quadrant abdominal pains, tachycardia, and mild hypotension. Laboratory tests revealed severe anemia and leukocytosis. The abdominal CT scan demonstrated dilation of the biliopancreatic limb and excluded stomach, with an intraluminal hyperdense lesion proximal to the jejunojejunal anastomosis. Laparoscopy revealed an intraluminal hematoma obstructing the biliopancreatic limb, secondary to a hemorrhage from the excluded stomach. Revision of the jejunojenunal anastomosis, hematoma evacuation, gastrostomy of the excluded stomach, and drainage were performed. Two days later, the patient developed recurrent abdominal pain with the apparition of bile in the drainage. A laparoscopy was performed and revealed a staple line dehiscence of the excluded stomach, requiring resection of its proximal portion. The postoperative course was complicated by a retrogastric hematoma and a peri-gastrojejunal abscess requiring laparoscopic lavage, drainage and closure of the gastrostomy. The remainder post-operative period was uneventful.

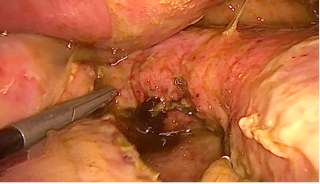

Abdominal Intercostal Hernias : A Case Series of Four Patients
Abstract
Background
Abdominal intercostal hernias (AIHs) are a rare and often misdiagnosed clinical entity characterized by protrusion of abdominal viscera through an intercostal space under an intact diaphragm. Due to its rarity and nonspecific presentation, diagnosis is often delayed, potentially leading to serious complications including incarceration and strangulation.
Aims
This short case series aims to describe the clinical features, diagnostic approach, and surgical management of AIHs, and to contribute to the limited literature on this rare condition.
Methods
We present a retrospective analysis of four patients diagnosed and treated for abdominal intercostal hernias at our institution between December 12th 2023 and January 1st 2026. Patient demographics, etiology, clinical presentation, imaging findings, surgical technique, and postoperative outcomes were analyzed.
Results
The series included four males (mean age = 69). Etiologies were traumatic (n=3) and spontaneous (n=1). Intercostal defects were mainly located at the 9th intercostal space (n=2). The most common presenting symptoms were chest wall swelling (n=4) and pain (n=3). CT imaging confirmed the diagnosis in all cases, demonstrating herniation of digestive organs (omentum, small bowel, or colon) through the intercostal defect with intact diaphragm. Three patients underwent open surgical repair with mesh reinforcement. Operative repair was not performed in one patient due to comorbidities and age. Mean operative time was 89 minutes with no major intraoperative complications. Mean hospital stay was 5.6 days. During a mean follow-up of 5.8 months, one patient presented with persistent AIH due to initial misdiagnosis as a flank hernia, highlighting the diagnostic and therapeutic challenge of this rare entity.
Conclusion
Abdominal intercostal hernia should be suspected in patients presenting with inferior chest bulging, particularly following minor or major trauma. CT imaging is essential for accurate diagnosis and surgical planning. Early recognition and prompt surgical intervention are crucial to prevent potentially life-threatening complications.
Herniation of the small bowel through the foramen of Winslow: A case report
Abstract
Background
Foramen of Winslow hernia (FWH) is a rare clinical situation, accounting for approximately 8% of internal hernias and only 0.08% of all hernias. Clinical diagnosis is challenging due to aspecific symptoms, and CT scan is essential for early diagnosis. Optimal surgical management remain debated. We report a case of small bowel herniation through the foramen of Winslow.
Conclusion
FWH is a rare pathology presenting with nonspecific symptoms and diagnosed by abdominal CT scan. Emergency laparoscopy is a safe and effective approach, even in the presence of bowel ischemia. Routine closure of the foramen of Winslow is debated to prevent recurrence and may expose patients to serious complications, including portal vein thrombosis or iatrogenic injury to the portal trial. Surgical strategy should therefore be individualized. In the present case, cholecystectomy allowed for widening and loosening of the foramen.
Case presentation
A 49-year-old man with a history of umbilical hernia repair without mesh presented to the emergency department with isolated epigastric pain evolving for 12 hours. Physical examination revealed epigastric guarding, while laboratory tests showed no inflammatory response. Abdominal CT scan suggested an internal hernia through the foramen of Winslow with signs of small bowel ischemia. Emergency exploratory laparoscopy revealed dilated small bowel herniating through a narrow foramen of Winslow. After reduction, indocyanine green fluorescence angiography demonstrated adequate bowel perfusion, allowing bowel preservation. Given the narrow foramen, a cholecystectomy was performed to achieve an adequate widening of the foramen (video available). The postoperative course was uneventful, with oral intake resumed on day 0. The patient was discharged on day 3, with no recurrence of symptoms reported.

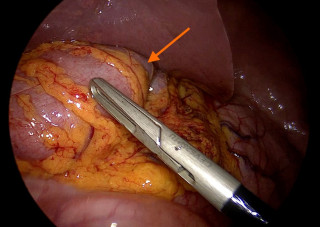
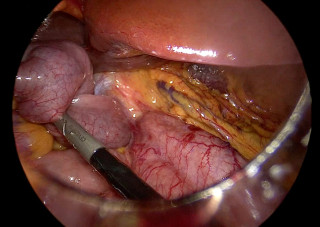
Post-Traumatic Hepatic Pseudoaneurysm: A Case Report
Abstract
Background
Traumatic hepatic pseudoaneurysms are rare complications of blunt liver injury. Despite initial hemodynamic stability, they may rupture suddenly, causing potentially fatal hemorrhage. Early CT follow-up is essential. Treatment options include endovascular embolization, ultrasound-guided thrombin injection, angiographic stent placement, surgical ligation, or hepatic resection.
Aims
To document the clinical course, imaging findings, and management of traumatic hepatic-pseudoaneurysms, a rare but potentially life-threatening complication of liver trauma.
Methods
A retrospective analysis of a patient with traumatic hepatic pseudoaneurysms was performed. Clinical presentation, laboratory findings, imaging, management, and follow-up were reviewed. Contrast-enhanced CT was used for diagnosis and surveillance. Liver injury severity was graded according to the American Association for the Surgery of Trauma (AAST) liver injury scale.
Results
A young adult patient presented with right upper quadrant pain after a high-energy traffic accident, remaining hemodynamically stable. Laboratory tests revealed mild anemia and markedly elevated transaminases (> eightfold increase). CT revealed a grade III perihilar liver laceration in segment V with three arterial pseudoaneurysms, one in segment V (7 mm) and two in segment VIII (5 mm, 6 mm) (Figure 1). No active bleeding or free fluid was detected.
Follow-up CT at 48 hours showed stable laceration but enlargement of the segment V pseudoaneurysm to 11 mm. Selective segmental coil embolization was successfully performed (Figure 2 and 3). Eight-week follow-up CT showed complete exclusion of the treated pseudoaneurysm, regression of remaining segment VIII pseudoaneurysms, and resolution of the laceration.
Conclusion
Post-traumatic hepatic pseudoaneurysms may enlarge and rupture unpredictably, even in clinically stable patients. Routine imaging surveillance is essential. Selective endovascular embolization represents an effective and organ-preserving prophylactic treatment strategy, potentially reducing liver-related complications compared with non-selective arterial embolization.
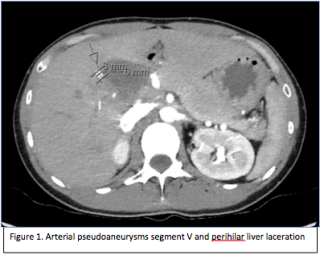
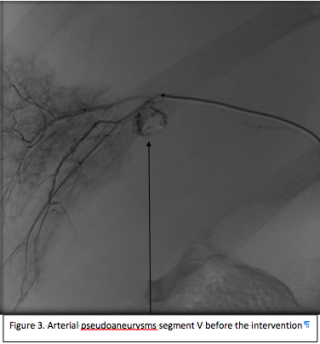
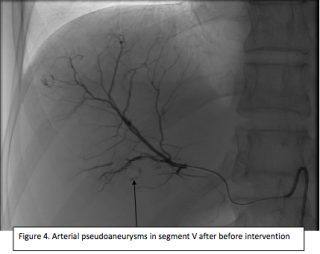
Acute Gastric And Distal Oesophageal Necrosis Secondary To Idiopathic Portal Vein Thrombosis: A Rare Surgical Emergency.
Abstract
Background
Acute gastric necrosis is an exceptionally rare and catastrophic condition due to the stomach’s extensive vascular supply. Most reported cases are related to arterial insufficiency, gastric volvulus, or caustic injury. Venous outflow obstruction, particularly secondary to portal vein thrombosis (PVT), represents an exceedingly uncommon mechanism and remains sparsely described. Acute PVT can abruptly impair gastric venous drainage, resulting in severe venous congestion, oedema, reduced mucosal perfusion, and progression to transmural necrosis. Because of its rarity and non-specific presentation, gastric venous ischemia is frequently under-recognized with delaying diagnosis and treatment.
Conclusion
This case highlights acute gastric necrosis as a rare, life-threatening, and under-recognized complication of portal vein thrombosis. Gastric necrosis should not be attributed exclusively to arterial ischemia, as venous outflow obstruction alone may precipitate catastrophic injury. Contrast-enhanced CT is essential for early detection of vascular thrombosis and ischemic gastric changes, while histopathological findings of diffuse venous congestion and transmural necrosis support a venous ischemic mechanism. Early anticoagulation and prompt surgical intervention are critical when full-thickness necrosis is present. Awareness of gastric venous ischemia broadens the differential diagnosis of acute abdominal pain and hematemesis and may improve patient outcomes.
Case presentation
A 56-year-old woman with no prior surgery or prothrombotic risk factors presented with acute abdominal pain and hematemesis. Contrast-enhanced CT showed extensive splanchnic venous thrombosis involving the portal vein trunk, intrahepatic branches, splenomesenteric confluence, and splenic vein, with marked hypoenhancement of the gastric fundus and greater curvature. Emergency laparoscopy revealed diffuse gastric and distal oesophageal necrosis, requiring conversion to open surgery. Total gastrectomy with transhiatal distal oesophagectomy and Roux-en-Y esophagojejunal anastomosis was performed with prophylactic intraluminal EndoSponge placement. Antimicrobial therapy, anticoagulation, and endoscopic therapy led to recovery. Thrombophilia investigations were negative, confirming idiopathic vein thrombosis.
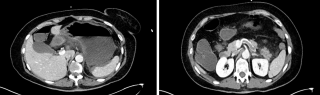
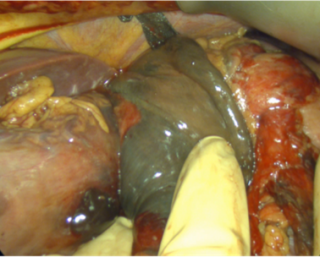
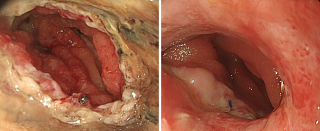
Register here for the course day (10.06.26) and the congress days (11./12.06.26)






